

Persistently Elevated Glucagon-Like Peptide-1 Levels among Critically Ill Surgical Patients after Sepsis and Development of Chronic Critical Illness and Dismal Long-Term Outcomes
- PMID: 30991107
- PMCID: PMC6599553
- DOI: 10.1016/j.jamcollsurg.2019.04.014
Persistently Elevated Glucagon-Like Peptide-1 Levels among Critically Ill Surgical Patients after Sepsis and Development of Chronic Critical Illness and Dismal Long-Term Outcomes
Abstract
Background: Glucagon-like peptide-1 (GLP-1) is a gut-derived incretin hormone that stimulates insulin secretion, cellular glucose uptake, and has immune-regulatory functions. Glucagon-like peptide-1 is markedly altered after trauma and sepsis, but the implications remain unclear.
Study design: We performed an analysis of a prospective, longitudinal cohort study of critically ill surgical patients with sepsis. Patient characteristics and clinical data were collected, as well as peripheral blood sampling for biomarker analysis, out to 28 days after sepsis onset. We prospectively adjudicated sepsis diagnosis, severity, clinical outcomes, and 6-month follow-up.
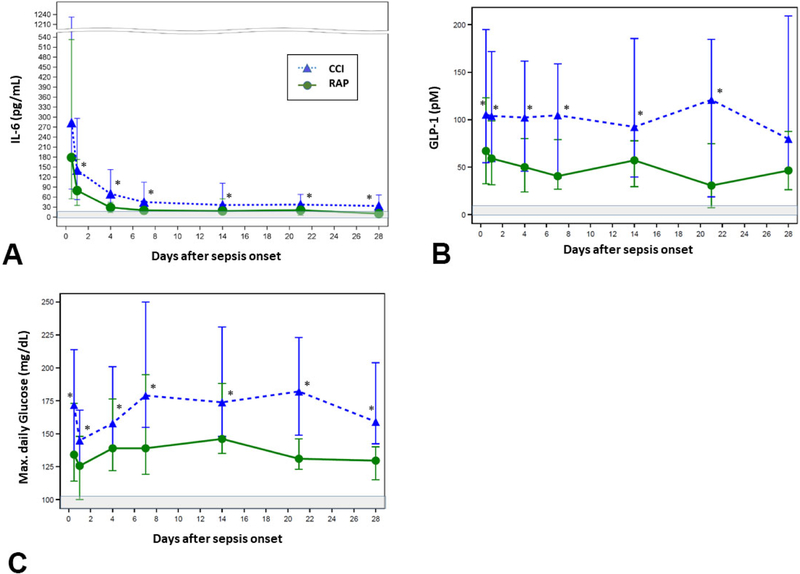
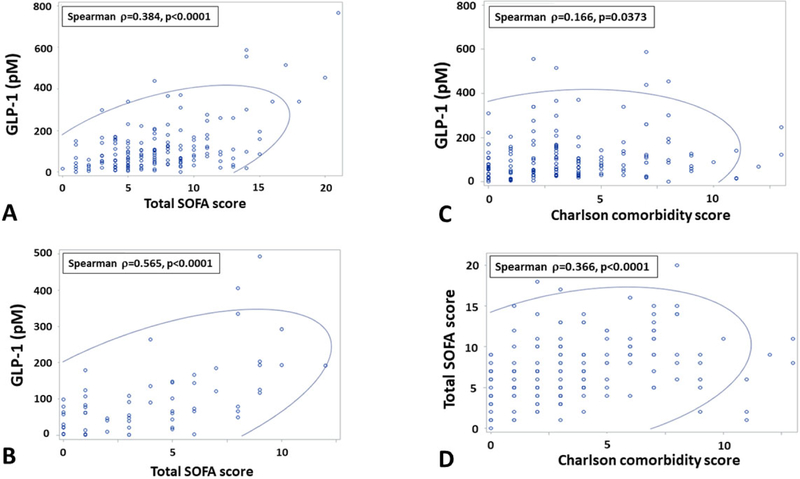
Results: The cohort included 157 septic surgical patients with significant physiologic derangement (Maximum Sequential Organ Failure Assessment [SOFA] score 8, interquartile range [IQR] 4 to 11), a high rate of multiple organ failure (50.3%), and septic shock (24.2%). Despite high disease severity, both early death (<14 days; n = 4, 2.9%) and overall inpatient mortality were low (n = 12, 7.6%). However, post-discharge 6-month mortality was nearly 3-fold higher (19.7%). Both GLP-1 and interleukin [IL]-6 levels were significantly elevated for 21 days (p ≤ 0.01) in patients who developed chronic critical illness (CCI) compared with patients with a rapid recovery. Elevated GLP-1 at 24 hours was a significant independent predictor for the development of CCI after controlling for IL-6 and glucose levels (p = 0.027), and at day 14 for death or severe functional disability at 6 months (WHO/Zubrod score 4-5, p = 0.014).
Conclusions: Elevated GLP-1 within 24 hours of sepsis is a predictor of early death or persistent organ dysfunction. Among early survivors, persistently elevated GLP-1 levels at day 14 are strongly predictive of death or severe functional disability at 6 months. Persistently elevated GLP-1 levels may be a marker of a nonresolving catabolic state that is associated with muscle wasting and dismal outcomes after sepsis and chronic critical illness.
Trial registration: ClinicalTrials.gov NCT02276417.
Copyright © 2019 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Discussion.J Am Coll Surg. 2019 Jul;229(1):67-68. doi: 10.1016/j.jamcollsurg.2019.05.013. J Am Coll Surg. 2019. PMID: 31248526 No abstract available.
References
-
- Yendamuri S, Fulda GJ, Tinkoff G. Admission hyperglycemia as a prognostic indicator in trauma. J Trauma 2003; 55: 33–38. - PubMed
-
- Laird AM, Miller PR, Kilgo PD, et al. Relationship of early hyperglycemia to mortality in trauma patients. J Trauma 2004; 56: 1058–62. - PubMed
-
- Bochcchio GV, Sung J, Joshi M, et al. Persistent hyperglycemia is predictive of outcome in critically ill trauma patients. J Trauma 2005; 58: 921–24. - PubMed
-
- Vanhorebeek, Langouche L, Van den Berghe G. Tight blood glucose control: what is the evidence? Crit Care Med 2007; S496–502. - PubMed
-
- Van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. N Engl J Med 2001; 345: 1359–67. - PubMed
