

Chest wall thickness and depth to vital structures in paediatric patients - implications for prehospital needle decompression of tension pneumothorax
- PMID: 30992028
- PMCID: PMC6469218
- DOI: 10.1186/s13049-019-0623-5
Chest wall thickness and depth to vital structures in paediatric patients - implications for prehospital needle decompression of tension pneumothorax
Abstract
Background: Recommendations regarding decompression of tension pneumothorax in small children are scarce and mainly transferred from the adult literature without existing evidence for the paediatric population. This CT-based study evaluates chest wall thickness, width of the intercostal space (ICS) and risk of injury to vital structures by needle decompression in children.
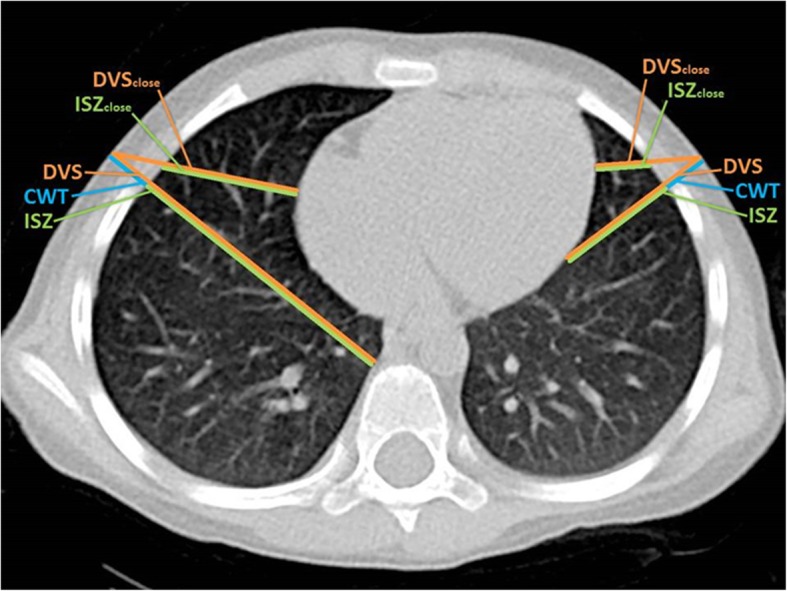
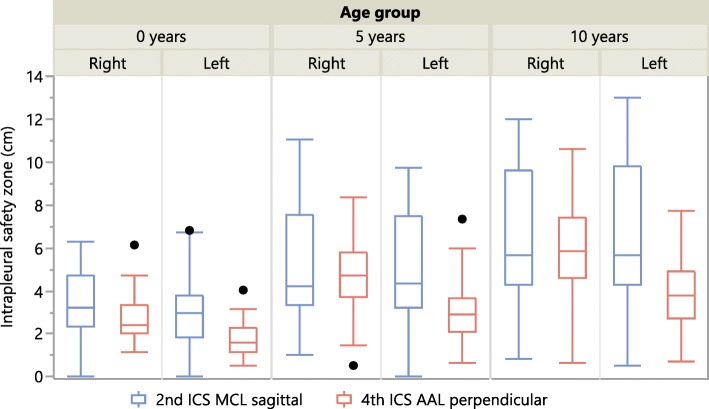
Methods: Chest wall thickness, width of the intercostal space and depth to vital structures were measured and evaluated at 2nd ICS midclavicular (MCL) line and 4th ICS anterior axillary line (AAL) on both sides of the thorax using computed tomography (CT) in 139 children in three different age groups (0, 5, 10 years).
Results: Width of the intercostal space was significantly smaller at the 4th ICS compared to the 2nd ICS in all age groups on both sides of the thorax. Chest wall thickness was marginally smaller at the 4th ICS compared to the 2nd ICS in infants and significantly smaller at 4th ICS in children aged 5 years and 10 years. Depth to vital structure for correct angle of needle entry was smaller at the 4th ICS in all age groups on both sides of the thorax. Incorrect angle of needle entry however is accompanied by a higher risk of injury at 2nd ICS. Furthermore, in some children aged 0 and 5 years, the heart or the thymus gland were found directly adjacent to the thoracic wall at 2nd ICS midclavicular line.
Conclusion: Especially in small children risk of iatrogenic injury to vital structures by needle decompression is considerably high. The 4th ICS AAL offers a smaller chest wall thickness, but the width of the ICS is smaller and the risk of injury to the intercostal vessels and nerve is greater. Deviations from correct angle of entry however are accompanied by higher risk of injury to intrathoracic structures at the 2nd ICS. Furthermore, we found the heart and the thymus gland to be directly adjacent to the thoracic wall at the 2nd ICS MCL in a few children. From our point of view this puncture site can therefore not be recommended for decompression in small children. We therefore recommend 4th ICS AAL as the primary site of choice.
Keywords: Chest wall thickness; Children; Complications; Needle decompression; Paediatric; Tension pneumothorax.
Conflict of interest statement
Authors’ information
All authors work at Mannheim University Medical Center. TT, TV, MR and MS work as consultants in anesthesiology and prehospital emergency medicine, with a strong focus on paediatric anesthesiology and paediatric emergency medicine. GL is writing his doctoral thesis on decompression of tension pneumothorax in children. LW is head of the Department of Paediatric Surgery and a well-known expert in paediatric traumatology and paediatric thoracic surgery. MW and HH are radiology consultants with a focus on cardiothoracic imaging and paediatric radiology.
Ethics approval and consent to participate
Ethics approval for this study was obtained from Medical Ethics Committee II, Medical Faculty Mannheim, Mannheim University (Reference number: 2013-818R-MA).
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- American College of Surgeons. Advanced trauma life support ®, 9th ed. Chicago: American College of Surgeons; 2013.
-
- Bouillon B, Begleitung M, Pieper D et al. S3 – Leitlinie Polytrauma / Schwerverletzten-Behandlung. AWMF Register-Nr. 012/019. 2016. https://www.awmf.org/uploads/tx_szleitlinien/012-019l_S3_Polytrauma_Schw....
-
- Montgomery HR, Butler FK, Giebner SD et al. TACTICAL COMBAT CASUALTY CARE (TCCC / TC3) https://rmf.ims.allogy.com/pf.tlx/Z03ZHMZHr5TL. Accessed 20 Nov 2018.
-
- American College of Surgeons. Advanced Trauma Life Support ®, 10th ed. Chicago: American College of Surgeons; 2018.
-
- Advanced Life Support Group. Advanced Pediatric Life Support, 6th Edition. Hoboken: Wiley-Blackwell; 2016.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
