

Heterogeneity of regional inflection points from pressure-volume curves assessed by electrical impedance tomography
- PMID: 30992054
- PMCID: PMC6469223
- DOI: 10.1186/s13054-019-2417-6
Heterogeneity of regional inflection points from pressure-volume curves assessed by electrical impedance tomography
Abstract
Background: The pressure-volume (P-V) curve has been suggested as a bedside tool to set mechanical ventilation; however, it reflects a global behavior of the lung without giving information on the regional mechanical properties. Regional P-V (PVr) curves derived from electrical impedance tomography (EIT) could provide valuable clinical information at bedside, being able to explore the regional mechanics of the lung. In the present study, we hypothesized that regional P-V curves would provide different information from those obtained from global P-V curves, both in terms of upper and lower inflection points. Therefore, we constructed pressure-volume curves for each pixel row from non-dependent to dependent lung regions of patients affected by acute hypoxemic respiratory failure (AHRF) and acute respiratory distress syndrome (ARDS).
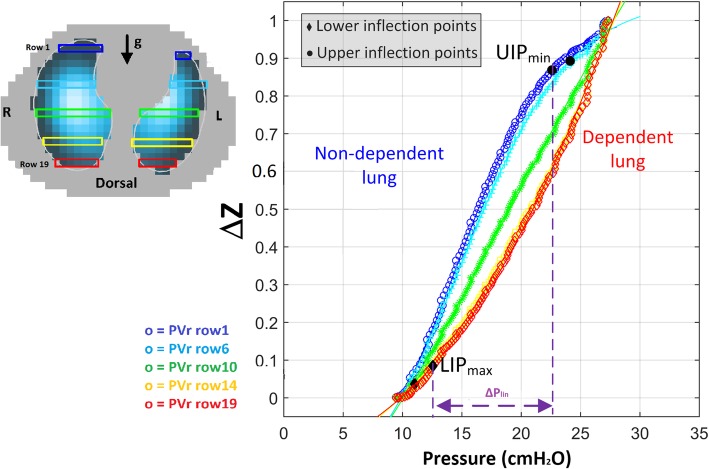
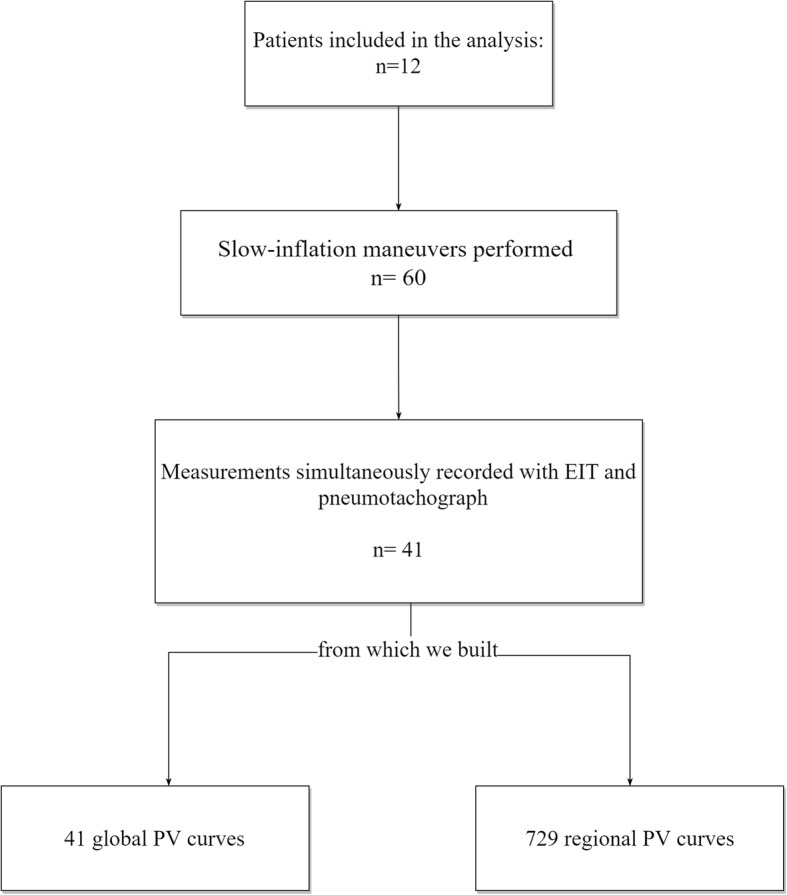
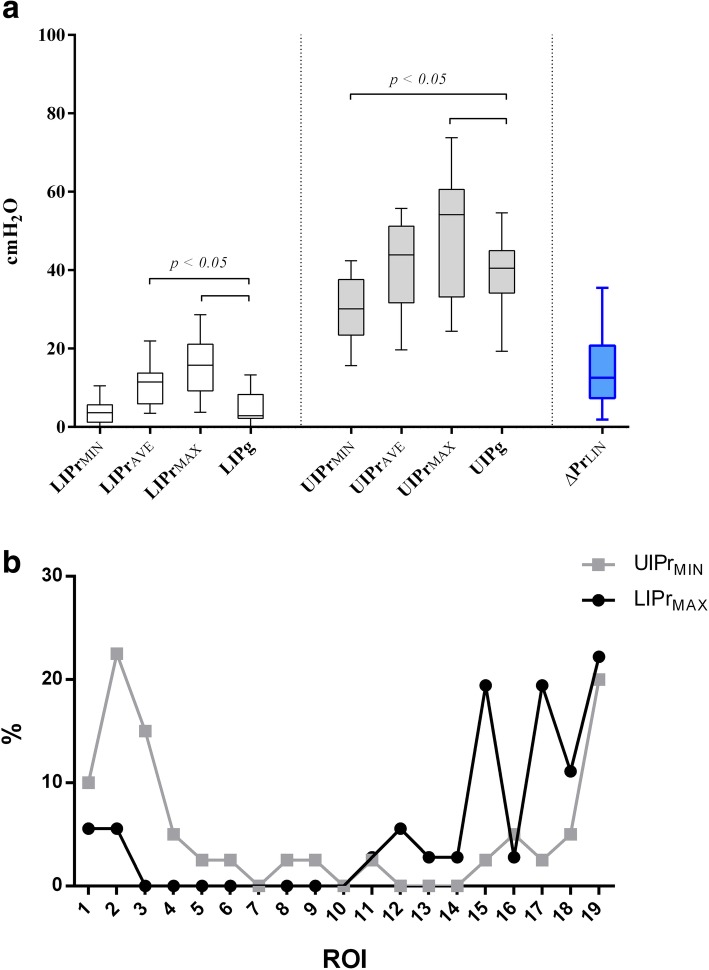
Methods: We analyzed slow-inflation P-V maneuvers data from 12 mechanically ventilated patients. During the inflation, the pneumotachograph was used to record flow and airway pressure while the EIT signals were recorded digitally. From each maneuver, global respiratory system P-V curve (PVg) and PVr curves were obtained, each one corresponding to a pixel row within the EIT image. PVg and PVr curves were fitted using a sigmoidal equation, and the upper (UIP) and lower (LIP) inflection points for each curve were mathematically identified; LIP and UIP from PVg were respectively called LIPg and UIPg. From each measurement, the highest regional LIP (LIPrMAX) and the lowest regional UIP (UIPrMIN) were identified and the pressure difference between those two points was defined as linear driving pressure (ΔPLIN).
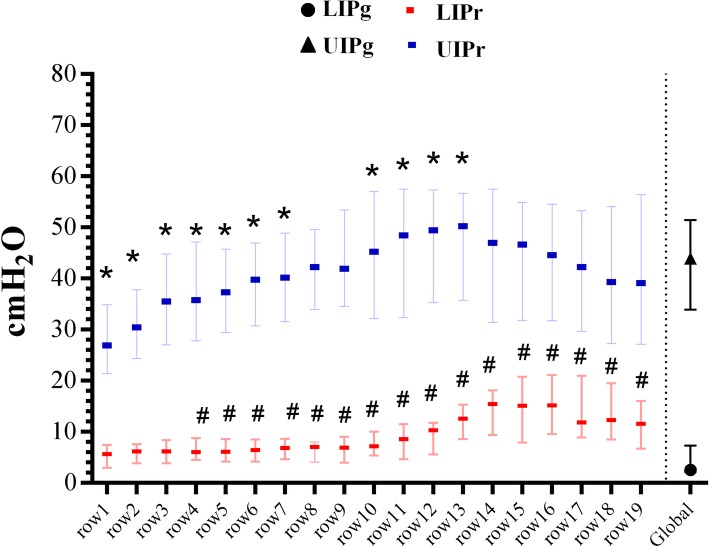
Results: A significant difference (p < 0.001) was found between LIPrMAX (15.8 [9.2-21.1] cmH2O) and LIPg (2.9 [2.2-8.9] cmH2O); in all measurements, the LIPrMAX was higher than the corresponding LIPg. We found a significant difference (p < 0.005) between UIPrMIN (30.1 [23.5-37.6] cmH2O) and UIPg (40.5 [34.2-45] cmH2O), the UIPrMIN always being lower than the corresponding UIPg. Median ΔPLIN was 12.6 [7.4-20.8] cmH2O and in 56% of cases was < 14 cmH2O.
Conclusions: Regional inflection points derived by EIT show high variability reflecting lung heterogeneity. Regional P-V curves obtained by EIT could convey more sensitive information than global lung mechanics on the pressures within which all lung regions express linear compliance.
Trial registration: Clinicaltrials.gov, NCT02907840 . Registered on 20 September 2016.
Keywords: Acute respiratory failure, acute respiratory distress syndrome; Electrical impedance tomography; Mechanical ventilation; Personalized medicine; Pressure-volume curve.
Conflict of interest statement
Ethics approval and consent to participate
This manuscript is a secondary analysis of data coming from a prospective trial. The study was approved by the ethics committee of the Sant’ Anna Hospital, Ferrara, Italy (Protocol n. 141285).
Consent for publication
Written informed consent was obtained from the patients or their relatives for publication of their individual details. The consent forms are help by the authors and are available for review by the editor-in-chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Variation of poorly ventilated lung units (silent spaces) measured by electrical impedance tomography to dynamically assess recruitment.Crit Care. 2018 Jan 31;22(1):26. doi: 10.1186/s13054-017-1931-7. Crit Care. 2018. PMID: 29386048 Free PMC article. Clinical Trial.
-
Regional pulmonary pressure volume curves in mechanically ventilated patients with acute respiratory failure measured by electrical impedance tomography.Acta Anaesthesiol Scand. 2006 Mar;50(3):331-9. doi: 10.1111/j.1399-6576.2006.00958.x. Acta Anaesthesiol Scand. 2006. PMID: 16480467
-
Distribution of airway pressure opening in the lungs measured with electrical impedance tomography (POET): a prospective physiological study.Crit Care. 2025 Jan 16;29(1):28. doi: 10.1186/s13054-025-05264-3. Crit Care. 2025. PMID: 39819779 Free PMC article. Clinical Trial.
-
How respiratory system mechanics may help in minimising ventilator-induced lung injury in ARDS patients.Eur Respir J Suppl. 2003 Aug;42:15s-21s. doi: 10.1183/09031936.03.00420303. Eur Respir J Suppl. 2003. PMID: 12945996 Review.
-
Electrical impedance tomography: A compass for the safe route to optimal PEEP.Respir Med. 2021 Oct;187:106555. doi: 10.1016/j.rmed.2021.106555. Epub 2021 Jul 30. Respir Med. 2021. PMID: 34352563 Review.
Cited by
-
Clinical Features and Outcomes of Acute Kidney Injury in Critically Ill COVID-19 Patients: A Retrospective Observational Study.J Clin Med. 2023 Aug 4;12(15):5127. doi: 10.3390/jcm12155127. J Clin Med. 2023. PMID: 37568528 Free PMC article.
-
Electrical impedance tomography monitoring in adult ICU patients: state-of-the-art, recommendations for standardized acquisition, processing, and clinical use, and future directions.Crit Care. 2024 Nov 19;28(1):377. doi: 10.1186/s13054-024-05173-x. Crit Care. 2024. PMID: 39563476 Free PMC article. Review.
-
Decades Under the Influence: Shifting the PEEP Paradigm in ARDS.Respir Care. 2024 Sep 26;69(10):1347-1350. doi: 10.4187/respcare.12435. Respir Care. 2024. PMID: 39327024 No abstract available.
-
Inter-lung asymmetrical airway closure cause insufflation delay between lungs in acute hypoxemic respiratory failure.Ann Intensive Care. 2024 Oct 23;14(1):162. doi: 10.1186/s13613-024-01379-y. Ann Intensive Care. 2024. PMID: 39441425 Free PMC article.
-
Gravitational distribution of regional opening and closing pressures, hysteresis and atelectrauma in ARDS evaluated by electrical impedance tomography.Crit Care. 2020 Oct 22;24(1):622. doi: 10.1186/s13054-020-03335-1. Crit Care. 2020. PMID: 33092607 Free PMC article.
References
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
