

Prostate-only Versus Whole-pelvis Radiation with or Without a Brachytherapy Boost for Gleason Grade Group 5 Prostate Cancer: A Retrospective Analysis
- PMID: 30992160
- PMCID: PMC7521828
- DOI: 10.1016/j.eururo.2019.03.022
Prostate-only Versus Whole-pelvis Radiation with or Without a Brachytherapy Boost for Gleason Grade Group 5 Prostate Cancer: A Retrospective Analysis
Abstract
Background: The role of elective whole-pelvis radiotherapy (WPRT) remains controversial. Few studies have investigated it in Gleason grade group (GG) 5 prostate cancer (PCa), known to have a high risk of nodal metastases.
Objective: To assess the impact of WPRT on patients with GG 5 PCa treated with external-beam radiotherapy (EBRT) or EBRT with a brachytherapy boost (EBRT+BT).
Design, setting, and participants: We identified 1170 patients with biopsy-proven GG 5 PCa from 11 centers in the United States and one in Norway treated between 2000 and 2013 (734 with EBRT and 436 with EBRT+BT).
Outcome measurements and statistical analysis: Biochemical recurrence-free survival (bRFS), distant metastasis-free survival (DMFS), and prostate cancer-specific survival (PCSS) were compared using Cox proportional hazards models with propensity score adjustment.
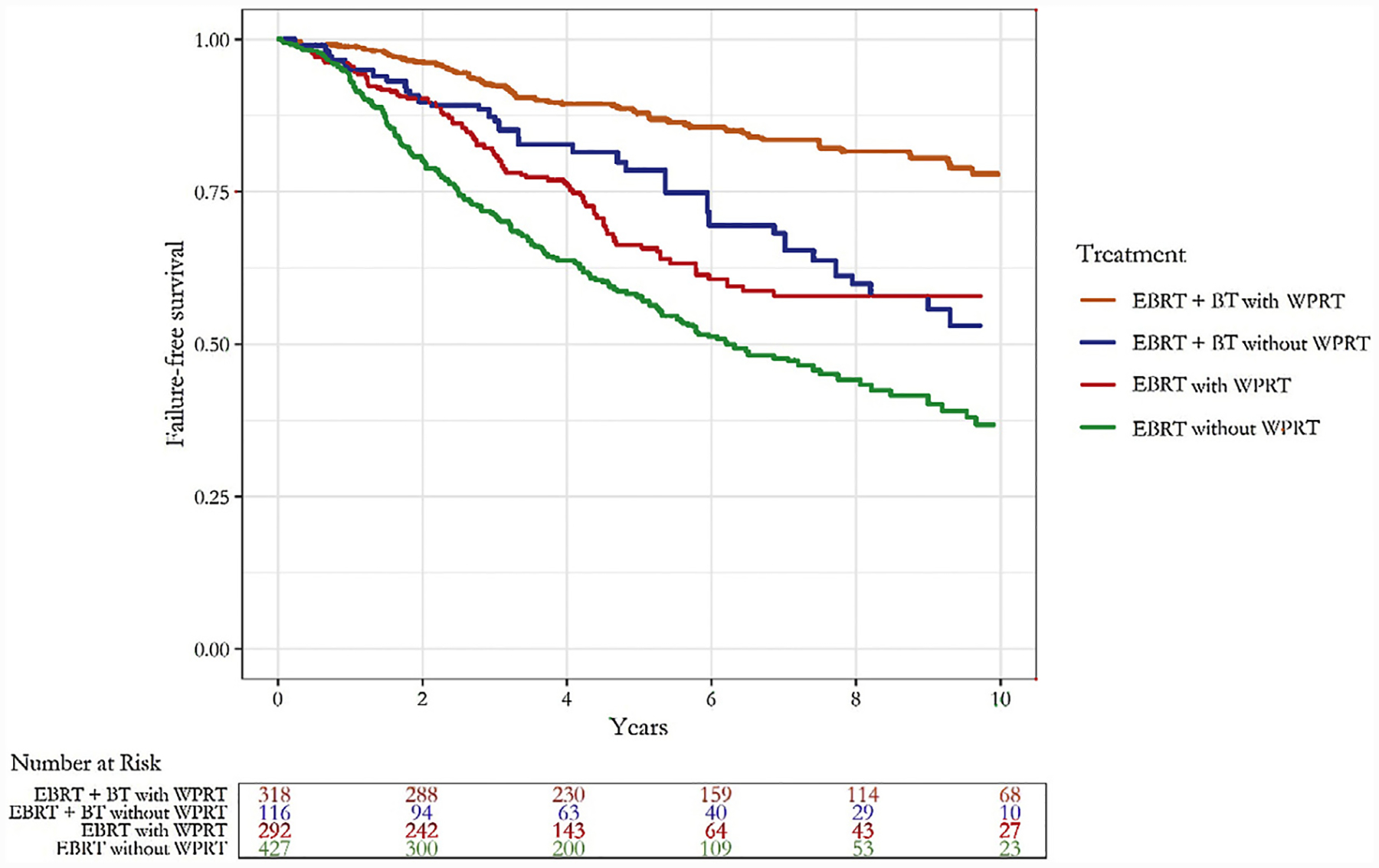
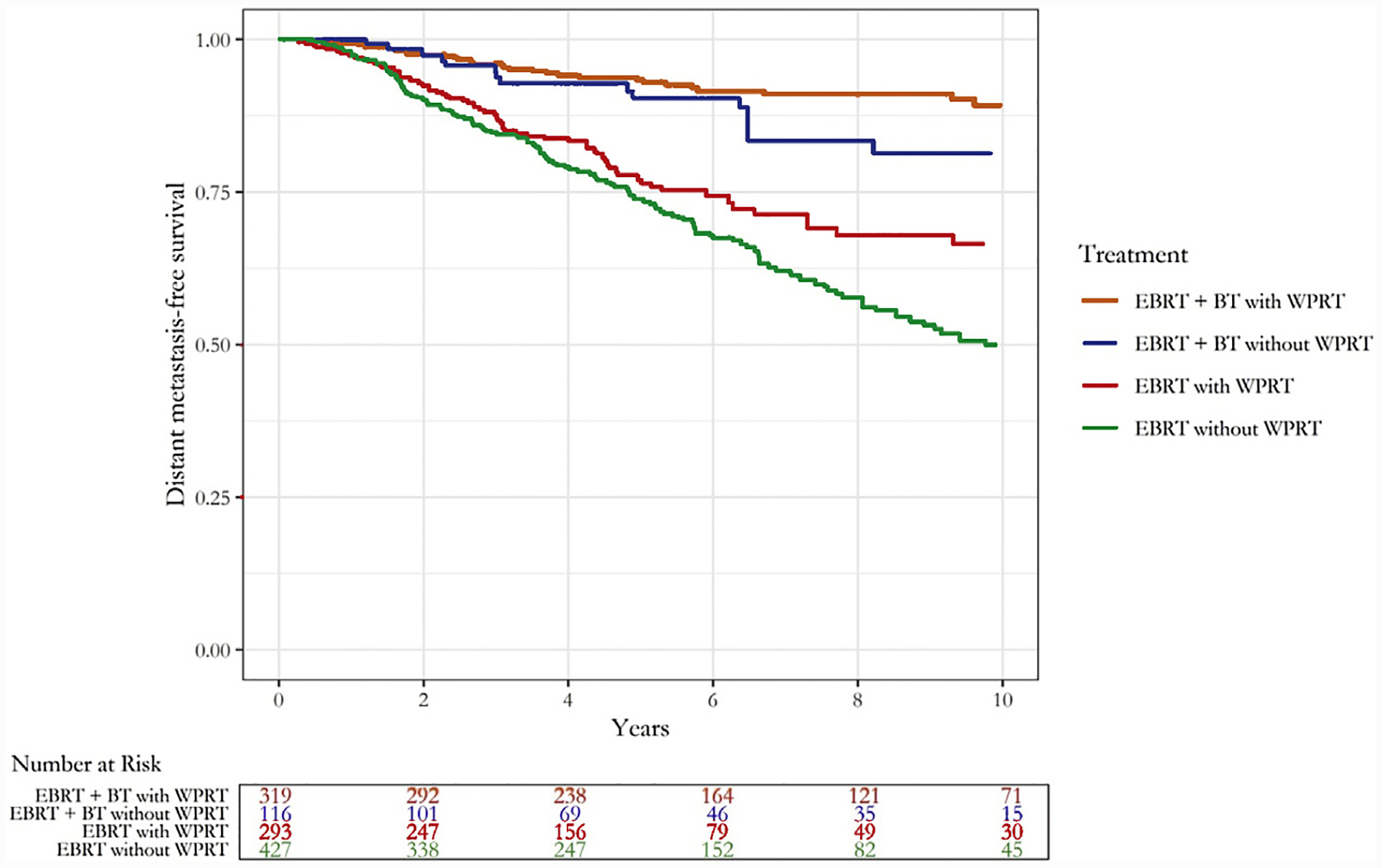
Results and limitations: A total of 299 EBRT patients (41%) and 320 EBRT+BT patients (73%) received WPRT. The adjusted 5-yr bRFS rates with WPRT in the EBRT and EBRT+BT groups were 66% and 88%, respectively. Without WPRT, these rates for the EBRT and EBRT+BT groups were 58% and 78%, respectively. The median follow-up was 5.6yr. WPRT was associated with improved bRFS among patients treated with EBRT+BT (hazard ratio [HR] 0.5, 95% confidence interval [CI] 0.2-0.9, p=0.02), but no evidence for improvement was found in those treated with EBRT (HR 0.8, 95% CI 0.6-1.2, p=0.4). WPRT was not significantly associated with improved DMFS or PCSS in the EBRT group (HR 1.1, 95% CI 0.7-1.7, p=0.8 for DMFS and HR 0.7, 95% CI 0.4-1.1, p=0.1 for PCSS), or in the EBRT+BT group (HR 0.6, 95% CI 0.3-1.4, p=0.2 for DMFS and HR 0.5 95% CI 0.2-1.2, p=0.1 for PCSS).
Conclusions: WPRT was not associated with improved PCSS or DMFS in patients with GG 5 PCa who received either EBRT or EBRT+BT. However, WPRT was associated with a significant improvement in bRFS among patients receiving EBRT+BT. Strategies to optimize WPRT, potentially with the use of advanced imaging techniques to identify occult nodal disease, are warranted.
Patient summary: When men with a high Gleason grade prostate cancer receive radiation with external radiation and brachytherapy, the addition of radiation to the pelvis results in a longer duration of prostate-specific antigen control. However, we did not find a difference in their survival from prostate cancer or in their survival without metastatic disease. We also did not find a benefit for radiation to the pelvis in men who received radiation without brachytherapy.
Keywords: Brachytherapy; Gleason grade group 5; Prostate cancer; Radiation therapy; Whole-pelvis irradiation.
Copyright © 2019 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures

Comment in
-
Randomized Trials and the Goldilocks Problem.Eur Urol. 2020 Jan;77(1):11-13. doi: 10.1016/j.eururo.2019.05.002. Epub 2019 May 16. Eur Urol. 2020. PMID: 31103392 No abstract available.
-
Is pelvic prophylactic radiotherapy in prostate cancer just right?Transl Androl Urol. 2020 Oct;9(5):2296-2298. doi: 10.21037/tau-20-881. Transl Androl Urol. 2020. PMID: 33209698 Free PMC article. No abstract available.
References
-
- Nguyen PL, D’Amico AV. Targeting pelvic lymph nodes in men with intermediate- and high-risk prostate cancer despite two negative randomized trials. J Clin Oncol 2008;26:2055–6, [author reply 2056–7]. - PubMed
-
- Roach M 3rd, DeSilvio M, Lawton C, et al. Phase III trial comparing whole-pelvic versus prostate-only radiotherapy and neoadjuvant versus adjuvant combined androgen suppression: Radiation Therapy Oncology Group 9413. J Clin Oncol 2003;21:1904–11. - PubMed
-
- Lawton CA, DeSilvio M, Roach M 3rd, et al. An update of the phase III trial comparing whole pelvic to prostate only radiotherapy and neoadjuvant to adjuvant total androgen suppression: updated analysis of RTOG 94–13, with emphasis on unexpected hormone/radiation interactions. Int J Radiat Oncol Biol Phys 2007;69:646–55. - PMC - PubMed
-
- Morikawa LK, Roach M 3rd. Pelvic nodal radiotherapy in patients with unfavorable intermediate and high-risk prostate cancer: evidence, rationale, and future directions. Int J Radiat Oncol Biol Phys 2011;80:6–16. - PubMed
