

Optimizing treatment of HIV-associated lymphoma
- PMID: 30992269
- PMCID: PMC7493463
- DOI: 10.1182/blood-2018-01-791400
Optimizing treatment of HIV-associated lymphoma
Abstract
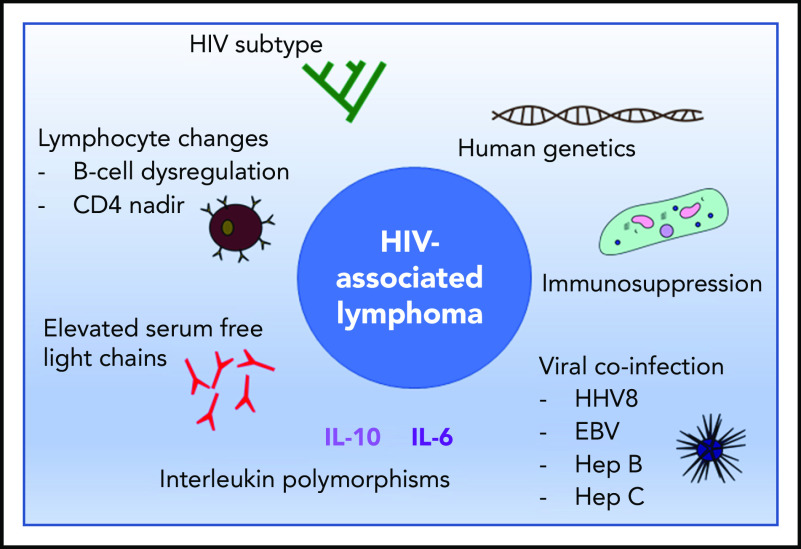
Cancer is the leading cause of death for HIV-infected persons in economically developed countries, even in the era of antiretroviral therapy (ART). Lymphomas remain a leading cause of cancer morbidity and mortality for HIV-infected patients and have increased incidence even in patients optimally treated with ART. Even limited interruptions of ART can lead to CD4 cell nadirs and HIV viremia, and increase the risk of lymphoma. The treatment of lymphoma is now similar for HIV-infected patients and the general population: patients with good HIV control can withstand intensive therapies appropriate to the lymphoma, including autologous and even allogeneic hematopoietic stem cell transplantation. Nonetheless, HIV-related lymphomas have unique aspects, including differences in lymphoma pathogenesis, driven by the presence of HIV, in addition to coinfection with oncogenic viruses. These differences might be exploited in the future to inform therapies. The relative incidences of lymphoma subtypes also differ in the HIV-infected population, and the propensity to advanced stage, aggressive presentation, and extranodal disease is higher. Other unique aspects include the need to avoid potential interactions between ART and chemotherapeutic agents, and the need for HIV-specific supportive care, such as infection prophylaxis. Despite these specific challenges for cancer treatment in the setting of HIV infection, the care of these patients has progressed sufficiently that recent guidelines from the American Society of Clinical Oncology advocate the inclusion of HIV-infected patients alongside HIV- patients in cancer clinical trials when appropriate.
© 2019 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: The author declares no competing financial interests.
Figures
References
-
- Lohse N, Obel N. Update of survival for persons with HIV infection in Denmark. Ann Intern Med. 2016;165(10):749-750. - PubMed
-
- Bower M, Palmieri C, Dhillon T. AIDS-related malignancies: changing epidemiology and the impact of highly active antiretroviral therapy. Curr Opin Infect Dis. 2006;19(1):14-19. - PubMed
-
- Patel P, Hanson DL, Sullivan PS, et al. ; Adult and Adolescent Spectrum of Disease Project and HIV Outpatient Study Investigators . Incidence of types of cancer among HIV-infected persons compared with the general population in the United States, 1992-2003. Ann Intern Med. 2008;148(10):728-736. - PubMed
-
- Puoti M, Bruno R, Soriano V, et al. ; HIV HCC Cooperative Italian-Spanish Group . Hepatocellular carcinoma in HIV-infected patients: epidemiological features, clinical presentation and outcome. AIDS. 2004;18(17):2285-2293. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
