

Laboratory validation of a clinical metagenomic sequencing assay for pathogen detection in cerebrospinal fluid
- PMID: 30992304
- PMCID: PMC6499319
- DOI: 10.1101/gr.238170.118
Laboratory validation of a clinical metagenomic sequencing assay for pathogen detection in cerebrospinal fluid
Abstract
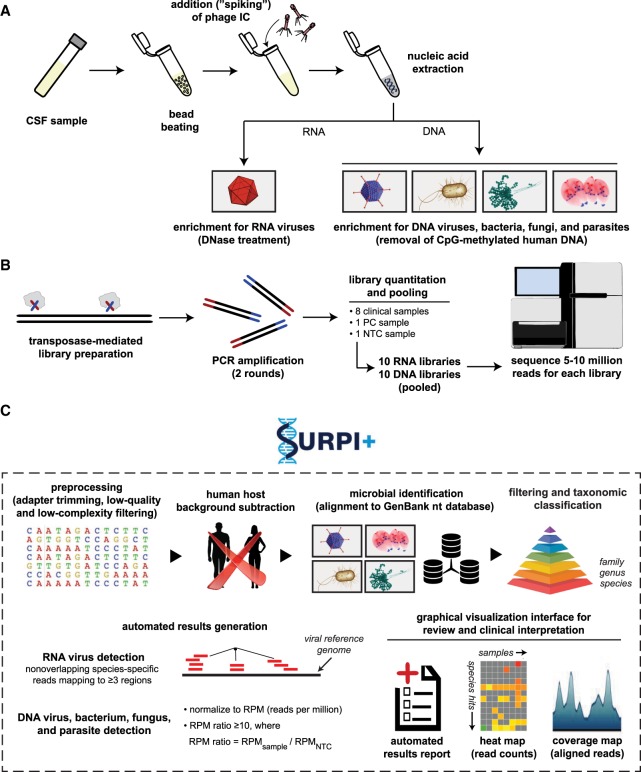
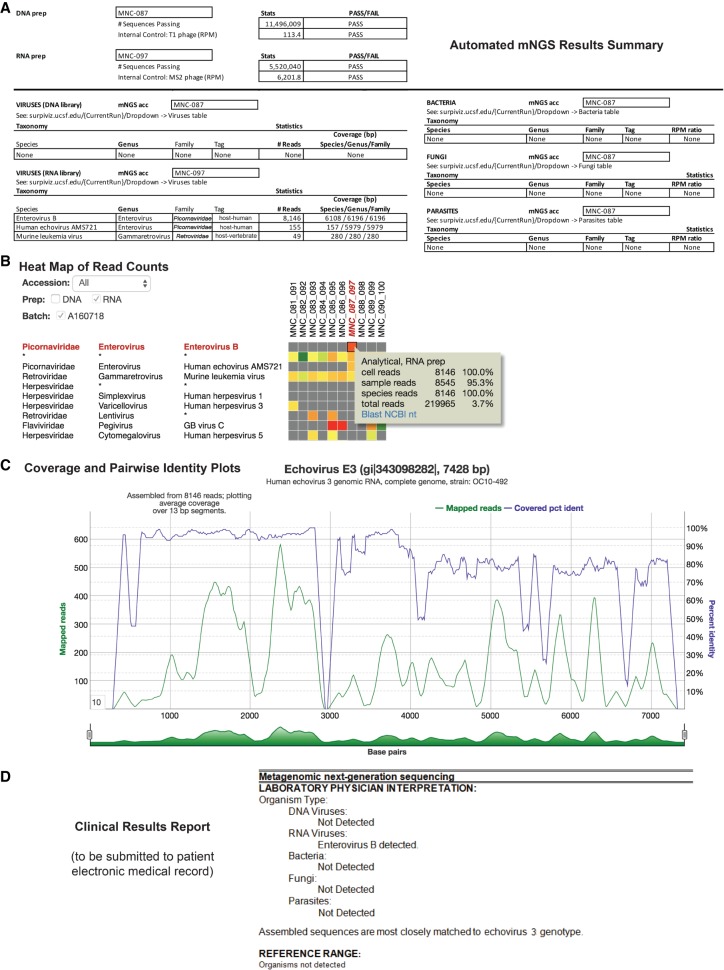
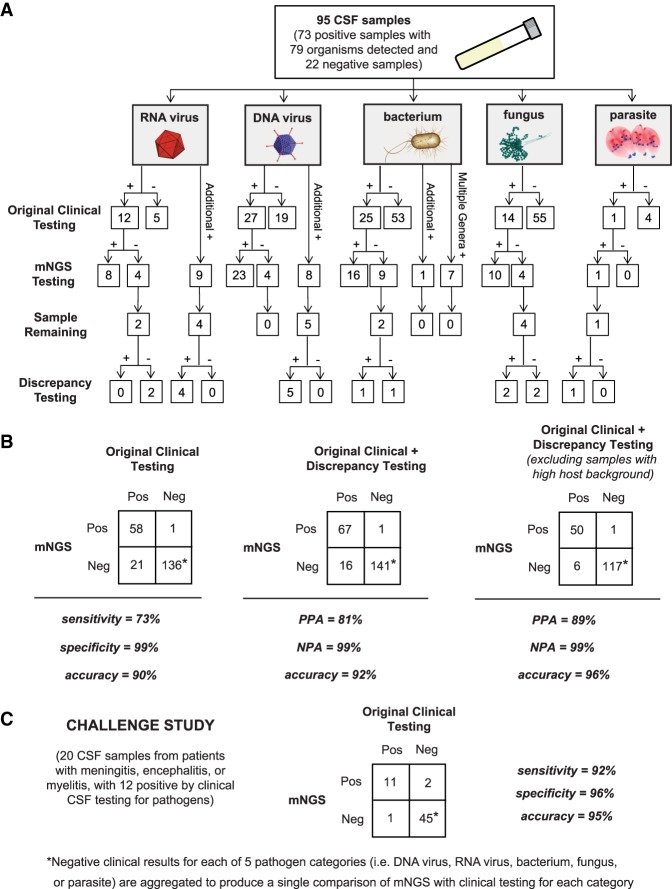
Metagenomic next-generation sequencing (mNGS) for pan-pathogen detection has been successfully tested in proof-of-concept case studies in patients with acute illness of unknown etiology but to date has been largely confined to research settings. Here, we developed and validated a clinical mNGS assay for diagnosis of infectious causes of meningitis and encephalitis from cerebrospinal fluid (CSF) in a licensed microbiology laboratory. A customized bioinformatics pipeline, SURPI+, was developed to rapidly analyze mNGS data, generate an automated summary of detected pathogens, and provide a graphical user interface for evaluating and interpreting results. We established quality metrics, threshold values, and limits of detection of 0.2-313 genomic copies or colony forming units per milliliter for each representative organism type. Gross hemolysis and excess host nucleic acid reduced assay sensitivity; however, spiked phages used as internal controls were reliable indicators of sensitivity loss. Diagnostic test accuracy was evaluated by blinded mNGS testing of 95 patient samples, revealing 73% sensitivity and 99% specificity compared to original clinical test results, and 81% positive percent agreement and 99% negative percent agreement after discrepancy analysis. Subsequent mNGS challenge testing of 20 positive CSF samples prospectively collected from a cohort of pediatric patients hospitalized with meningitis, encephalitis, and/or myelitis showed 92% sensitivity and 96% specificity relative to conventional microbiological testing of CSF in identifying the causative pathogen. These results demonstrate the analytic performance of a laboratory-validated mNGS assay for pan-pathogen detection, to be used clinically for diagnosis of neurological infections from CSF.
© 2019 Miller et al.; Published by Cold Spring Harbor Laboratory Press.
Figures
References
-
- Chiu C, Miller S. 2016. Next-generation sequencing. In Molecular microbiology: diagnostic princples and practice, 3rd ed. (ed. Persing DH, et al. ), pp. 68–79. ASM Press, Washington, DC.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases