

Review
doi: 10.1002/cld.655.
eCollection 2017 Sep.
The pathological differential diagnosis of portal hypertension
Affiliations
- PMID: 30992761
- PMCID: PMC6467111
- DOI: 10.1002/cld.655
Item in Clipboard
Review
The pathological differential diagnosis of portal hypertension
Clin Liver Dis (Hoboken).
.
No abstract available
Figures

Macroscopic and microscopic anatomy of the liver demonstrating blood flow. Level of obstruction leading to portal hypertension is identified by the letters corresponding to Table 1: (A) portal vein before entering the liver, (B) portal vein at the level of the portal tracts, (C) within the sinusoids, (D) at the juncture of the sinusoids and the central hepatic vein, and (E) hepatic vein outside the liver at the juncture of the vena cava.

Hepatoportal sclerosis demonstrated by a scarred area within the portal tract that is replacing the portal vein. A small lumen remains.

Schistosomiasis. (A) Portal tract demonstrating numerous calcified Schistosoma eggs imbedded within the portal vein and subsequent fibrosis . (B) Higher magnifications of calcified Schistosoma eggs.

Granulomatous hepatitis in a patient with sarcoidosis; a core biopsy demonstrates a prominent nonnecrotizing granuloma (oval) composed of coalescent macrophages with multinucleated giant cells (arrow).

Congenital hepatic fibrosis is characterized by broad fibrous septa, creating a geographic appearance with islands of hepatic parenchyma. The fibrous septa contain ductal structures that are reminiscent of bile duct hamartomas or Von Meyenburg complexes. This is in contrast with ductular proliferation, which is a physiological response to injury. Multiple bile duct hamartomas are typically present.

Amyloidosis of the liver with extensive deposition of amyloid (A) within the sinusoids compressing the hepatic plates (arrow).
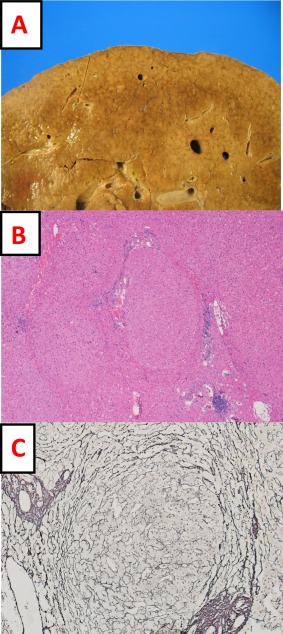
Nodular regenerative hyperplasia. (A) Gross photograph of a liver with diffuse nodularity. (B) Hematoxylin and eosin–stained section with nodular regeneration of hepatocytes without fibrosis. (C) Reticulin stain outlining a regenerative nodule with collapse of surrounding hepatic plates.

Veno‐occlusive disease (sinusoidal obstructive syndrome). A trichrome stain of the liver is shown that demonstrates fibrosis as blue. Two central veins are seen with reduced lumen size. The smaller vein shows obliteration of the lumen without complete scarring (red arrow). The larger central vein demonstrates a slit‐like lumen with dense fibrosis of the wall significantly reducing the lumen size (yellow arrow).
References
Publication types
LinkOut - more resources
Full Text Sources
