

Review
doi: 10.1002/cld.366.
eCollection 2014 Jun.
Budd-Chiari syndrome
Affiliations
- PMID: 30992907
- PMCID: PMC6448720
- DOI: 10.1002/cld.366
Item in Clipboard
Review
Budd-Chiari syndrome
Clin Liver Dis (Hoboken).
.
No abstract available
Figures

MRI of a Budd‐Chiari syndrome (BCS) liver (axial slice, T1, arterial phase after intravenous gadolinium chelate injection). The liver is heterogeneous. The three major hepatic veins (black arrows) appear as hypointense cords. Segment 1 is enlarged (white arrow heads). Courtesy of Maxime Ronot, MD.
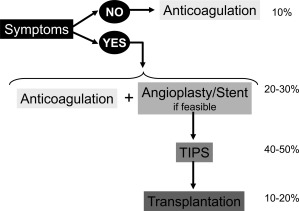
Proposed treatment strategy in patients with primary BCS. Numbers on the right represent the approximate proportion of patients who can be permanently controlled at each step of the strategy. Data are based on recent cohort studies.3, 4

Proposed algorithm for the management of hepatic nodules in BCS patients. In the context of BCS, the presence of liver nodule(s) with serum AFP level > 15 ng/ mL is highly suggestive of malignancy, and biopsy of the largest nodule should be performed to confirm the diagnosis of hepatocellular carcinoma (HCC). If serum AFP level is normal (< 15 ng/ mL), biopsy should be performed in heterogeneous nodules with diameter > 3 cm to rule out HCC. In patients with homogeneous nodules smaller than 3 cm and serum AFP level < 15 ng/ mL, an enhanced surveillance with 3‐month intervals should be performed in the first year after the initial nodule detection, followed by surveillance with 6‐month intervals if the lesion remains unchanged over this period.
References
-
- DC Valla. Primary Budd‐Chiari syndrome. J Hepatol 2009;50:195‐203. - PubMed
-
- S Darwish Murad, A Plessier, M Hernandez-Guerra, F Fabris, CE Eapen, MJ Bahr, et al. Etiology, management, and outcome of the Budd‐Chiari syndrome. Ann Intern Med 2009;151:167‐175. - PubMed
-
- S Seijo, A Plessier, J Hoekstra, A Dell'era, D Mandair, K Rifai, et al. Good long-term outcome of Budd‐Chiari syndrome with a step-wise management. Hepatology 2013;57:1962‐1968. - PubMed
-
- Chait Y, Condat B, Cazals‐Hatem D, Rufat P, Atmani S, Chaoui D, et al. Relevance of the criteria commonly used to diagnose myeloproliferative disorder in patients with splanchnic vein thrombosis. Br J Haematol 2005;129:553‐560. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
