

The Microbiome of Temporal Arteries
- PMID: 30993251
- PMCID: PMC6423729
- DOI: 10.20411/pai.v4i1.270
The Microbiome of Temporal Arteries
Abstract
Objective: A role for microorganisms in giant cell arteritis (GCA) has long been suspected. We describe the microbiomes of temporal arteries from patients with GCA and controls.
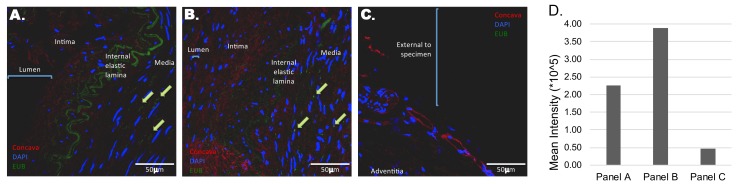
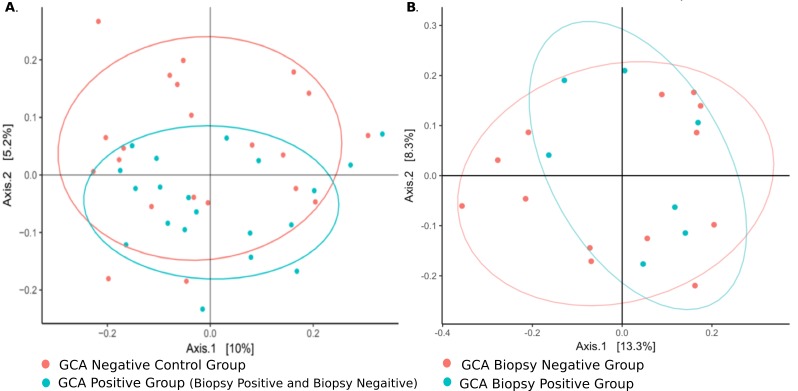
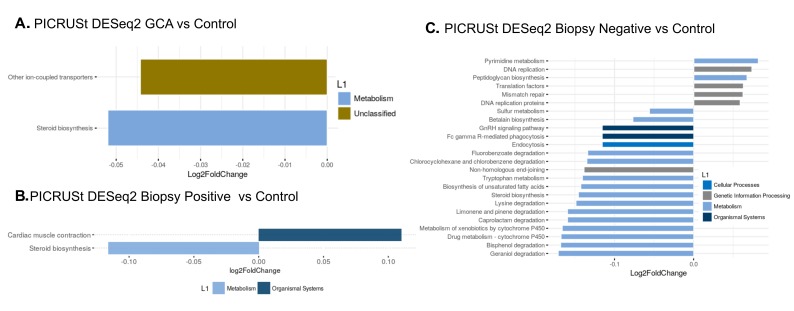
Methods: Temporal artery biopsies from patients suspected to have GCA were collected under aseptic conditions and snap-frozen. Fluorescence in situ hybridization (FISH) and long-read 16S rRNA-gene sequencing was used to examine microbiomes of temporal arteries. Taxonomic classification of bacterial sequences was performed to the genus level and relative abundances were calculated. Microbiome differential abundances were analyzed by principal coordinate analysis (PCoA) with comparative Unifrac distances and predicted functional profiling using PICRUSt.
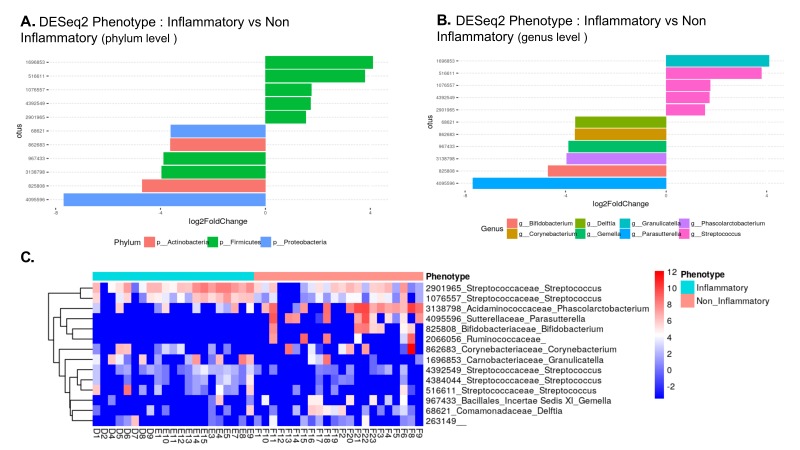
Results: Forty-seven patients, including 9 with biopsy-positive GCA, 15 with biopsy-negative GCA and 23 controls without GCA, were enrolled. FISH for bacterial DNA revealed signal in the arterial media. Beta, but not alpha, diversity differed between GCA and control temporal arteries (P = 0.042). Importantly, there were no significant differences between biopsy-positive and biopsy-negative GCA (P > 0.99). The largest differential abundances seen between GCA and non-GCA temporal arteries included Proteobacteria (P), Bifidobacterium (g), Parasutterella (g), and Granulicatella (g) [Log 2-fold change ≥ 4].
Conclusion: Temporal arteries are not sterile, but rather are inhabited by a community of bacteria. We have demonstrated that there are microbiomic differences between GCA and non-GCA temporal arteries, but not between biopsy-positive and biopsy-negative GCA.
Keywords: giant cell arteritis; microbiome; vasculitis.
Conflict of interest statement
Gary S. Hoffman and Leonard H. Calabrese are associate editors for Pathogens and Immunity. They did not participate in any aspect of the review or editorial process of this submitted manuscript.
Figures
References
-
- Prieto-Gonzalez S, Arguis P, Garcia-Martinez A, Espigol-Frigole G, Tavera-Bahillo I, Butjosa M, Sanchez M, Hernandez-Rodriguez J, Grau JM, Cid MC.. Large vessel involvement in biopsy-proven giant cell arteritis: prospective study in 40 newly diagnosed patients using CT angiography. Ann Rheum Dis. 2012;71(7):1170-6. PubMed PMID: 22267328. doi: 10.1136/annrheumdis-2011-200865 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources