

Diet and colorectal cancer in UK Biobank: a prospective study
- PMID: 30993317
- PMCID: PMC7124508
- DOI: 10.1093/ije/dyz064
Diet and colorectal cancer in UK Biobank: a prospective study
Abstract
Background: Most of the previous studies on diet and colorectal cancer were based on diets consumed during the 1990s.
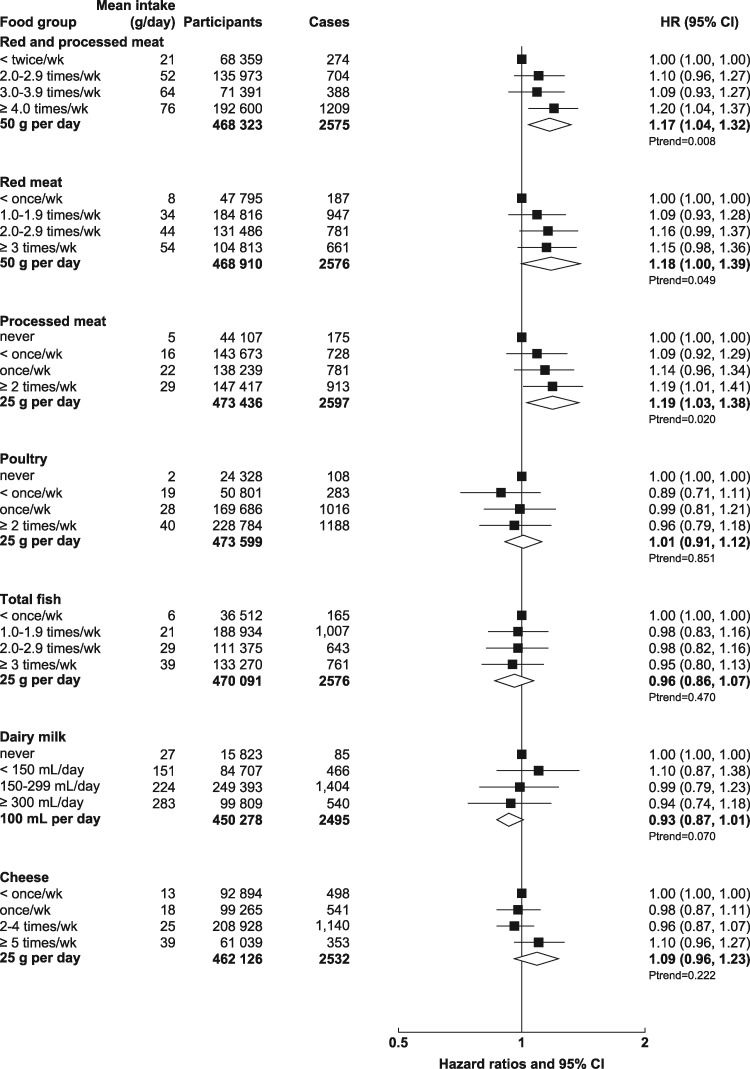
Methods: We used Cox-regression models to estimate adjusted hazard ratios for colorectal cancer by dietary factors in the UK Biobank study. Men and women aged 40-69 years at recruitment (2006-10) reported their diet on a short food-frequency questionnaire (n = 475 581). Dietary intakes were re-measured in a large sub-sample (n = 175 402) who completed an online 24-hour dietary assessment during follow-up. Trends in risk across the baseline categories were calculated by assigning re-measured intakes to allow for measurement error and changes in intake over time.
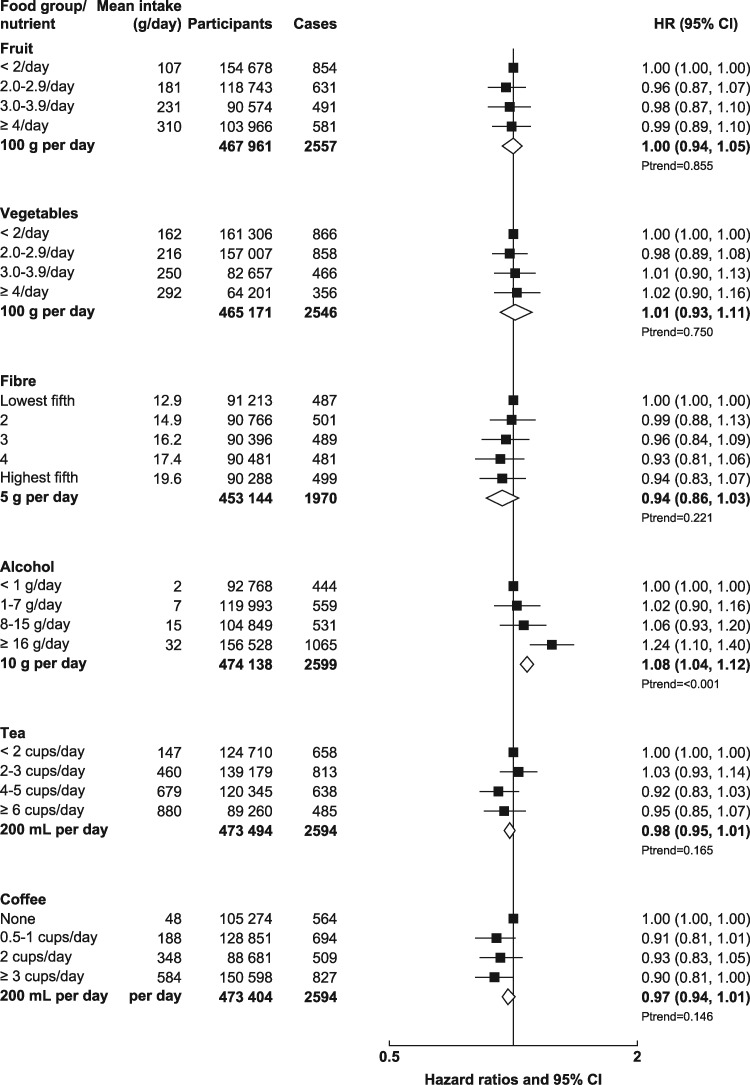
Results: During an average of 5.7 years of follow-up, 2609 cases of colorectal cancer occurred. Participants who reported consuming an average of 76 g/day of red and processed meat compared with 21 g/day had a 20% [95% confidence interval (CI): 4-37] higher risk of colorectal cancer. Participants in the highest fifth of intake of fibre from bread and breakfast cereals had a 14% (95% CI: 2-24) lower risk of colorectal cancer. Alcohol was associated with an 8% (95% CI: 4-12) higher risk per 10 g/day higher intake. Fish, poultry, cheese, fruit, vegetables, tea and coffee were not associated with colorectal-cancer risk.
Conclusions: Consumption of red and processed meat at an average level of 76 g/d that meets the current UK government recommendation (≤90 g/day) was associated with an increased risk of colorectal cancer. Alcohol was also associated with an increased risk of colorectal cancer, whereas fibre from bread and breakfast cereals was associated with a reduced risk.
Keywords: Diet; UK Biobank; colorectal cancer; processed meat; prospective study; red meat.
© The Author(s) 2019. Published by Oxford University Press on behalf of the International Epidemiological Association.
Figures
References
-
- Bouvard V, Loomis D, Guyton KZ. et al. Carcinogenicity of consumption of red and processed meat. Lancet Oncol 2015;16:1599–600. - PubMed
-
- World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Colorectal Cancer. Continuous Update Project Expert Report 2018 Available at dietandcancerreport.org.
-
- Kohlmeier L, Bellach B.. Exposure assessment error and its handling in nutritional epidemiology. Annu Rev Public Health 1995;16:43–59. - PubMed
-
- Willett W. Nutritional Epidemiology, 3rd edn.New York: Oxford University Press, 2013.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
