

Can we reduce the workload of mammographic screening by automatic identification of normal exams with artificial intelligence? A feasibility study
- PMID: 30993432
- PMCID: PMC6682851
- DOI: 10.1007/s00330-019-06186-9
Can we reduce the workload of mammographic screening by automatic identification of normal exams with artificial intelligence? A feasibility study
Abstract
Purpose: To study the feasibility of automatically identifying normal digital mammography (DM) exams with artificial intelligence (AI) to reduce the breast cancer screening reading workload.
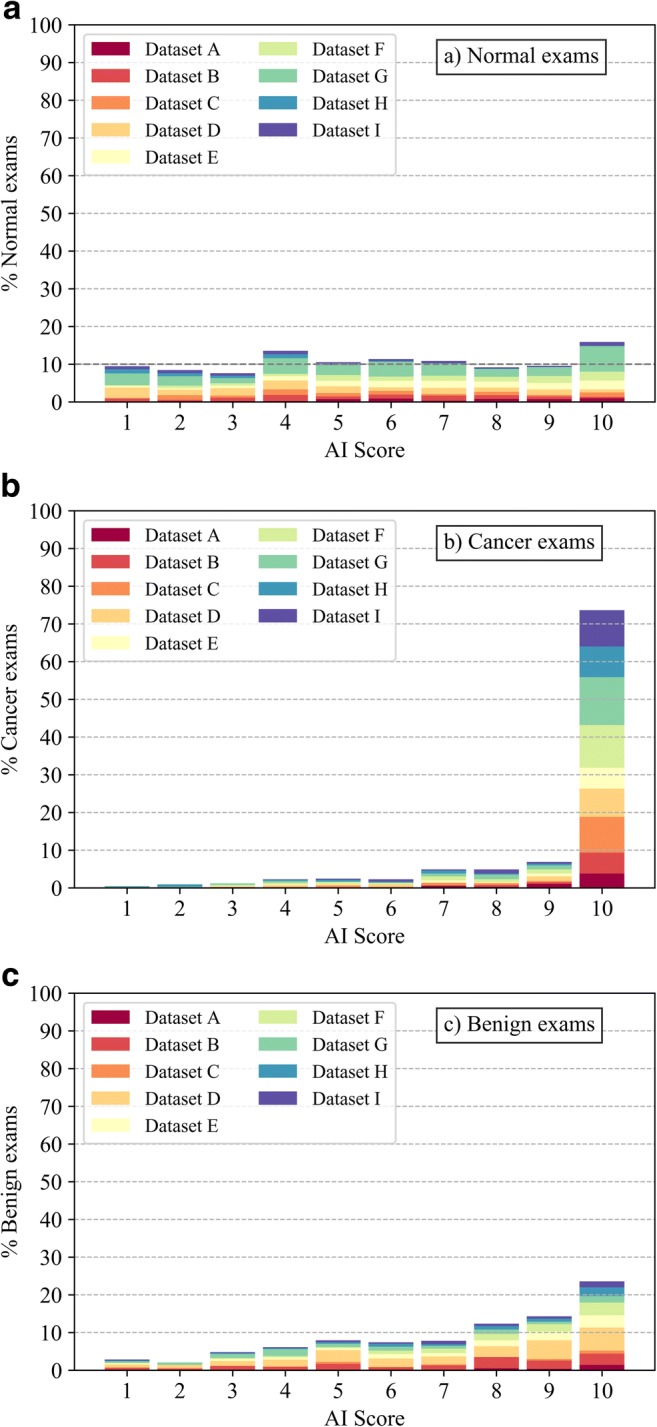
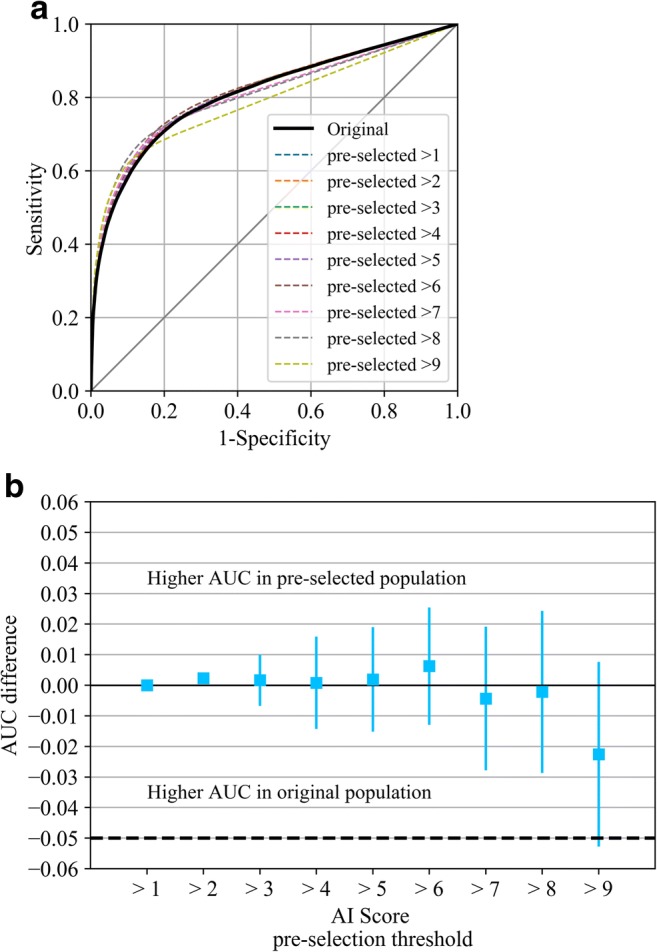
Methods and materials: A total of 2652 DM exams (653 cancer) and interpretations by 101 radiologists were gathered from nine previously performed multi-reader multi-case receiver operating characteristic (MRMC ROC) studies. An AI system was used to obtain a score between 1 and 10 for each exam, representing the likelihood of cancer present. Using all AI scores between 1 and 9 as possible thresholds, the exams were divided into groups of low- and high likelihood of cancer present. It was assumed that, under the pre-selection scenario, only the high-likelihood group would be read by radiologists, while all low-likelihood exams would be reported as normal. The area under the reader-averaged ROC curve (AUC) was calculated for the original evaluations and for the pre-selection scenarios and compared using a non-inferiority hypothesis.
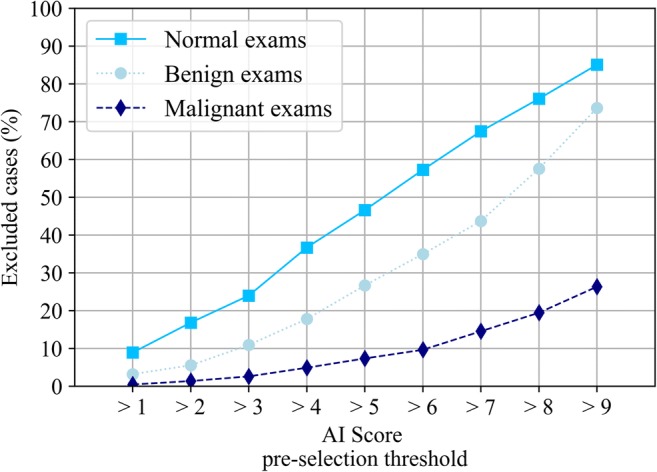
Results: Setting the low/high-likelihood threshold at an AI score of 5 (high likelihood > 5) results in a trade-off of approximately halving (- 47%) the workload to be read by radiologists while excluding 7% of true-positive exams. Using an AI score of 2 as threshold yields a workload reduction of 17% while only excluding 1% of true-positive exams. Pre-selection did not change the average AUC of radiologists (inferior 95% CI > - 0.05) for any threshold except at the extreme AI score of 9.
Conclusion: It is possible to automatically pre-select exams using AI to significantly reduce the breast cancer screening reading workload.
Key points: • There is potential to use artificial intelligence to automatically reduce the breast cancer screening reading workload by excluding exams with a low likelihood of cancer. • The exclusion of exams with the lowest likelihood of cancer in screening might not change radiologists' breast cancer detection performance. • When excluding exams with the lowest likelihood of cancer, the decrease in true-positive recalls would be balanced by a simultaneous reduction in false-positive recalls.
Keywords: Artificial intelligence; Breast cancer; Deep learning; Mammography; Screening.
Conflict of interest statement
The authors of this manuscript declare relationships with the following companies:
The authors KL, PC, TH, TM, SZ, IS, and RM of this manuscript declare relationships with Siemens Healthineers (Erlangen, Germany): TM is an employee, KL, PC, TH, SZ, IS, and RM received research grants.
The authors AR, AG, and RM declare relationships with ScreenPoint Medical BV (Nijmegen, Netherlands): AR and AG are employees, RM is an advisor.
Figures
References
-
- Breast Cancer Surveillance Consortium (BCSC) Performance measures for 1,838,372 screening mammography examinations from 2004 to 2008 by age–based on BCSC data through 2009. National Cancer Institute. Available via http://www.bcsc-research.org/statistics/performance/screening/2009/perf_.... Accessed 29 Sep 2017
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
