

Hepatic pleomorphic leiomyosarcoma after surgery for gastric gastrointestinal stromal tumor: a case report
- PMID: 30993477
- PMCID: PMC6468034
- DOI: 10.1186/s40792-019-0622-9
Hepatic pleomorphic leiomyosarcoma after surgery for gastric gastrointestinal stromal tumor: a case report
Abstract
Background: Pleomorphic leiomyosarcomas (PLMSs) are extremely rare tumors. We present the first case of hepatic primary PLMS after surgery for gastric gastrointestinal stromal tumor (GIST).
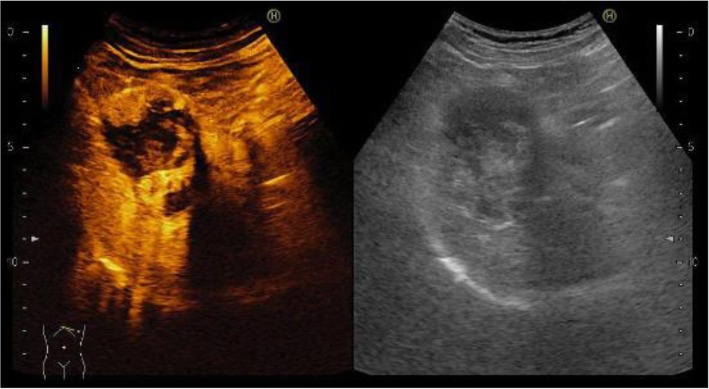
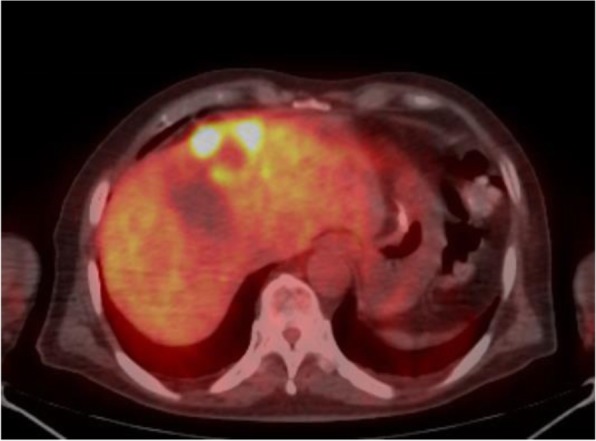
Case presentation: The patient was a 62-year-old man who was referred to our hospital for resection of a hepatic tumor arising after gastric GIST surgery that was resistant to imatinib and sunitinib. A 40-mm tumor in the left lobe of the liver and three small nodules in the right lobe were detected. We performed hepatic left lobectomy and partial resections for three lesions. According to the histopathological and immunohistochemical findings and c-kit gene mutations analysis, the main tumor was diagnosed as a PLMS.
Conclusion: It is necessary to consider the possibility that imatinib-resistant GIST recurrence lesions are a different kind of soft-tissue sarcoma. Accurate diagnosis is required to not miss the opportunity for radical excision of PLMS.
Keywords: Gastrointestinal stromal tumor; Hepatectomy; Pleomorphic hepatic leiomyosarcoma.
Conflict of interest statement
Consent for publication
Written informed consent was obtained from the patient for the publication of this case report and the accompanying images.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures





References
-
- Oda Y, Miyajima K, Kawaguchi K, Tamiya S, Oshiro Y, Hachitanda Y, et al. Pleomorphic leiomyosarcoma: clinicopathologic and immunohistochemical study with special emphasis on its distinction from ordinary leiomyosarcoma and malignant fibrous histiocytoma. Am J Surg Pathol. 2001;25(8):1030–1038. doi: 10.1097/00000478-200108000-00007. - DOI - PubMed
LinkOut - more resources
Full Text Sources
