

Left atrial longitudinal strain by speckle tracking as independent predictor of recurrence after electrical cardioversion in persistent and long standing persistent non-valvular atrial fibrillation
- PMID: 30993507
- PMCID: PMC6700045
- DOI: 10.1007/s10554-019-01597-7
Left atrial longitudinal strain by speckle tracking as independent predictor of recurrence after electrical cardioversion in persistent and long standing persistent non-valvular atrial fibrillation
Abstract
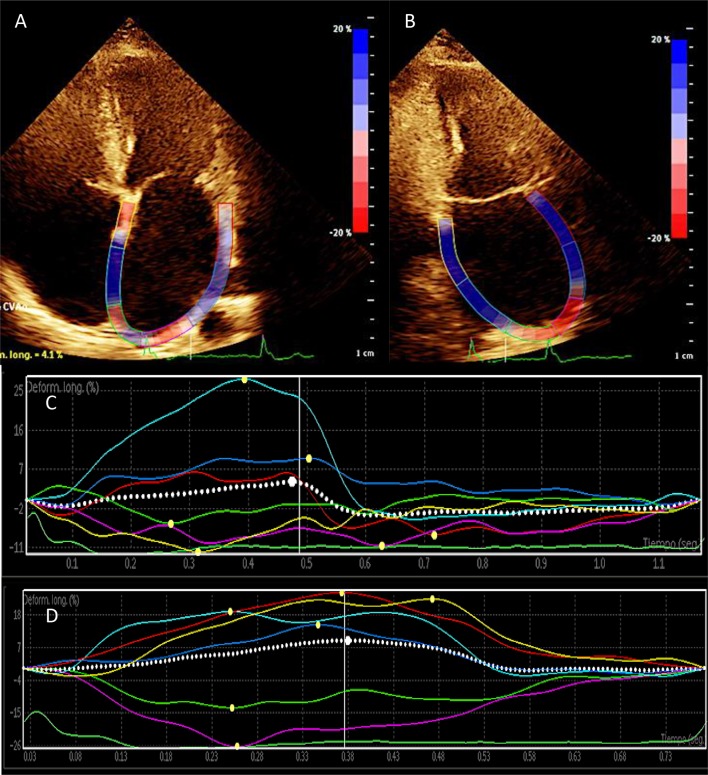
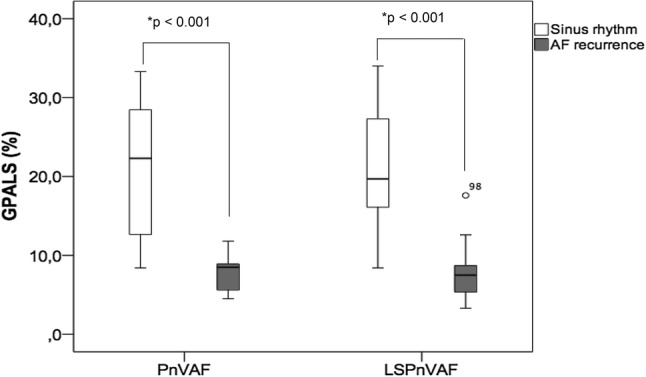
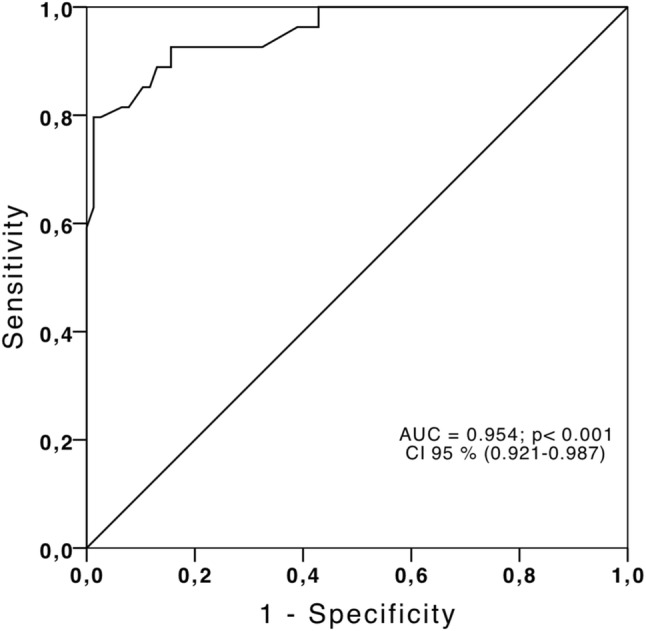
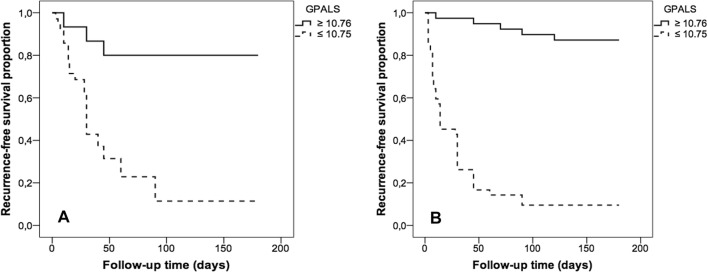
Atrial fibrillation (AF) is the most common arrhythmia in humans. After successful cardioversion, there is a recurrence of 60% due to atrial remodeling, and it has been shown that the global peak atrial longitudinal strain (GPALS) is decreased in these subjects. The aim of this study was to evaluate the predictive value of GPALS for AF recurrence. A prospective cohort of patients with persistent (PnVAF) and long standing persistent non-valvular AF (LSPnVAF) which underwent electrical cardioversion was evaluated with standard echocardiographic variables and GPALS quantification. The primary endpoint was AF recurrence at 6 months. We included PnVAF (n = 50, aged 68.4 ± 10.2 years, female 46%, lasted AF 6 months) and LSPnVAF (n = 81, aged 66.5 ± 13.1 years, female 36%, lasted AF 18 months). At 6 months there were a 68% of recurrence of AF in PnVAF and 53% in LSPnVAF group. GPALS was lower in recurrence 7.8 ± 2.0% versus 21.2 ± 8.9% (p < 0.001) for PnVAF and 7.3 ± 2.7% versus 20.7 ± 7.6% (p < 0.001) in LSPnVAF. GPALS ≤ 10.75% discriminates recurrence at 6 months with a sensitivity of 85%, specificity 99%, PPV 85%, NPV 90%, LR + 8.5 and LR- 0.17. The independent predictors of recurrence in PnVAF were GPALS ≤ 10.75% HR 8.89 [(2.2-35.7), p < 0.01] meanwhile in LSPnVAF were age HR 1.039 [(1.007-1.071), p = 0.01], and GPALS ≤ 10.75% HR 28.1 [(7.2-109.1), p < 0.001]. In subjects with PnVAF and LSPnVAF with successful electrical cardioversion, GPALS ≤ 10.75% predicts arrhythmia recurrence at 6-month follow-up.
Keywords: Atrial fibrillation; Longitudinal atrial strain; Recurrence.
Conflict of interest statement
All authors declare that they have no conflict of interest.
Figures
References
-
- Camm AJ, Kirchhof P, Lip GYH, Schotten U, Savelieva I, Ernst S, Van Gelder I, Al-Attar N, Hindricks G, Prendergast B, Heidbuchel H, Afieri O, Angelini A, Atar D, Colonna P, De Caterina R, De Sutter J, Goette A, Gorenek B, Heldal M, Hohloser SH, Kolh P, Le Heuzey JY, Ponikowski P, Rutten FH, ESC Committee for Practice Guidelines Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC) Eur Heart J. 2010;31:2369–2429. doi: 10.1093/eurheartj/ehq278. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
