

Use of Cardiac Computed Tomography and Magnetic Resonance Imaging in Case Management of Atrial Fibrillation with Catheter Ablation
- PMID: 30993921
- PMCID: PMC6470091
- DOI: 10.3348/kjr.2018.0774
Use of Cardiac Computed Tomography and Magnetic Resonance Imaging in Case Management of Atrial Fibrillation with Catheter Ablation
Abstract
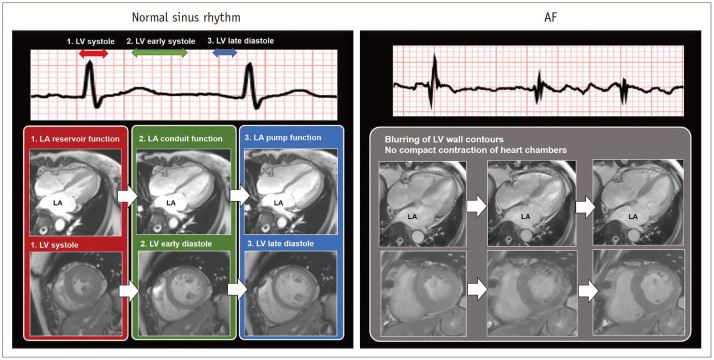
Atrial fibrillation (AF) is the most common arrhythmia associated with the risk of morbidity and mortality in clinical patients. AF is considered as an arrhythmia type that develops and progresses through close connection with cardiac structural arrhythmogenic substrates. Since the introduction of catheter ablation-mediated electrical isolation of arrhythmogenic substrates, cardiac imaging indicates improved treatment outcome and prognosis with appropriate candidate selection, ablation catheter guidance, and post-ablation follow-up. Currently, cardiac computed tomography (CCT) and cardiovascular magnetic resonance (CMR) imaging are essential in the case management of AF at both pre-and post-procedural stages of catheter ablation. In this review, we discuss the roles and technical considerations of CCT and CMR imaging in the management of patients with AF undergoing catheter ablation.
Keywords: Arrhythmia; Atrial fibrillation; Catheter ablation; Computed tomography; Magnetic resonance imaging.
Copyright © 2019 The Korean Society of Radiology.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
Similar articles
-
Comparison of cardiac computed tomography versus cardiac magnetic resonance for characterization of left atrium anatomy before radiofrequency catheter ablation of atrial fibrillation.Int J Cardiol. 2015 Jan 20;179:114-21. doi: 10.1016/j.ijcard.2014.10.030. Epub 2014 Nov 8. Int J Cardiol. 2015. PMID: 25464427
-
Catheter ablation of atrial fibrillation: cardiac imaging guidance as an adjunct to the electrophysiological guided approach.Europace. 2021 Apr 6;23(4):520-528. doi: 10.1093/europace/euaa249. Europace. 2021. PMID: 33555014 Review.
-
Multimodality imaging of left atrium in patients with atrial fibrillation.J Cardiovasc Comput Tomogr. 2019 Nov-Dec;13(6):340-346. doi: 10.1016/j.jcct.2019.03.005. Epub 2019 Mar 30. J Cardiovasc Comput Tomogr. 2019. PMID: 30952613 Review.
-
Sinus rhythm restores ventricular function in patients with cardiomyopathy and no late gadolinium enhancement on cardiac magnetic resonance imaging who undergo catheter ablation for atrial fibrillation.Heart Rhythm. 2013 Sep;10(9):1334-9. doi: 10.1016/j.hrthm.2013.06.019. Epub 2013 Jun 27. Heart Rhythm. 2013. PMID: 23811081
-
Magnetic resonance post-contrast T1 mapping in the human atrium: validation and impact on clinical outcome after catheter ablation for atrial fibrillation.Heart Rhythm. 2014 Sep;11(9):1551-9. doi: 10.1016/j.hrthm.2014.06.012. Epub 2014 Jun 12. Heart Rhythm. 2014. PMID: 24931636
Cited by
-
Guideline for Cardiovascular Magnetic Resonance Imaging from the Korean Society of Cardiovascular Imaging-Part 1: Standardized Protocol.Korean J Radiol. 2019 Sep;20(9):1313-1333. doi: 10.3348/kjr.2019.0398. Korean J Radiol. 2019. PMID: 31464111 Free PMC article.
-
Advancements in Imaging for Atrial Fibrillation Ablation: Is There a Potential to Improve Procedural Outcomes?J Innov Card Rhythm Manag. 2020 Jul 15;11(7):4172-4178. doi: 10.19102/icrm.2020.110701. eCollection 2020 Jul. J Innov Card Rhythm Manag. 2020. PMID: 32724708 Free PMC article. Review.
-
Guidelines for Cardiovascular Magnetic Resonance Imaging from the Korean Society of Cardiovascular Imaging-Part 2: Interpretation of Cine, Flow, and Angiography Data.Korean J Radiol. 2019 Nov;20(11):1477-1490. doi: 10.3348/kjr.2019.0407. Korean J Radiol. 2019. PMID: 31606953 Free PMC article. Review.
-
Evaluation of Left Atrial Appendage Isolation Using Cardiac MRI after Catheter Ablation of Atrial Fibrillation: Paradox of Appendage Reservoir.Korean J Radiol. 2021 Apr;22(4):525-534. doi: 10.3348/kjr.2020.0629. Epub 2020 Nov 19. Korean J Radiol. 2021. PMID: 33236545 Free PMC article.
-
Guidelines for Cardiovascular Magnetic Resonance Imaging from the Korean Society of Cardiovascular Imaging-Part 3: Perfusion, Delayed Enhancement, and T1- and T2 Mapping.Korean J Radiol. 2019 Dec;20(12):1562-1582. doi: 10.3348/kjr.2019.0411. Korean J Radiol. 2019. PMID: 31854146 Free PMC article. Review.
References
-
- January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, Jr, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2014;64:e1–e76. - PubMed
-
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37:2893–2962. - PubMed
-
- Aviles RJ, Martin DO, Apperson-Hansen C, Houghtaling PL, Rautaharju P, Kronmal RA, et al. Inflammation as a risk factor for atrial fibrillation. Circulation. 2003;108:3006–3010. - PubMed
-
- Nattel S, Allessie M, Haissaguerre M. Spotlight on atrial fibrillation-the ‘complete arrhythmia’. Cardiovasc Res. 2002;54:197–203. - PubMed
