

Development and Initial Validation of a Frontline Health Worker mHealth Assessment Platform (MEDSINC®) for Children 2-60 Months of Age
- PMID: 30994099
- PMCID: PMC6553915
- DOI: 10.4269/ajtmh.18-0869
Development and Initial Validation of a Frontline Health Worker mHealth Assessment Platform (MEDSINC®) for Children 2-60 Months of Age
Abstract
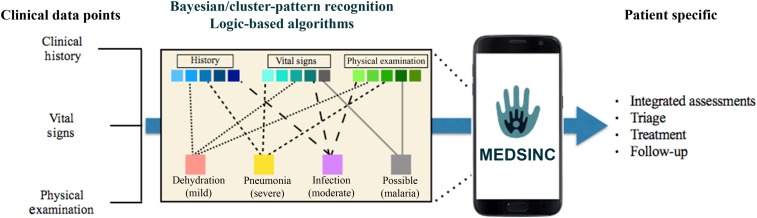
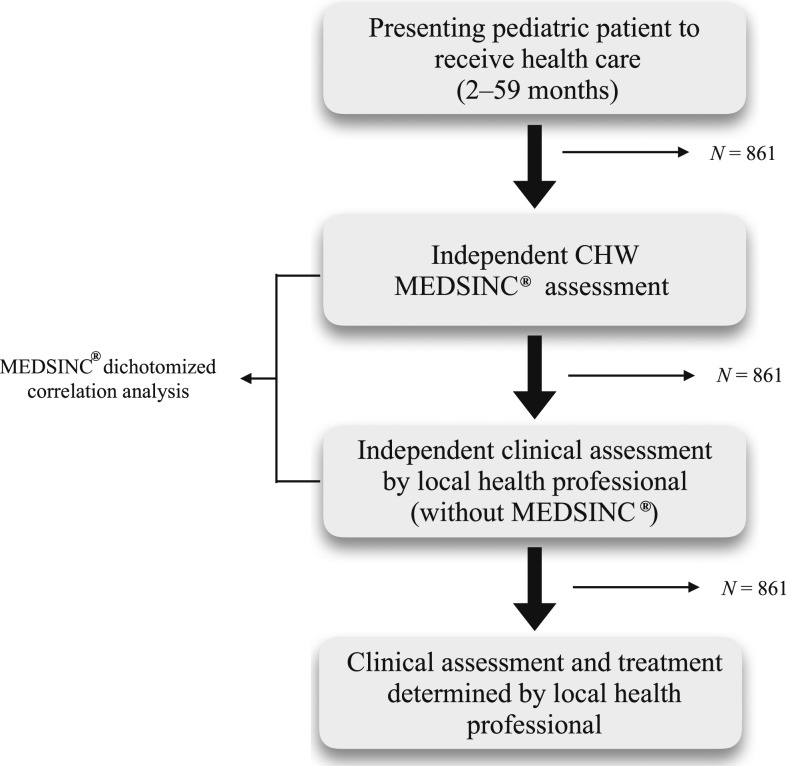
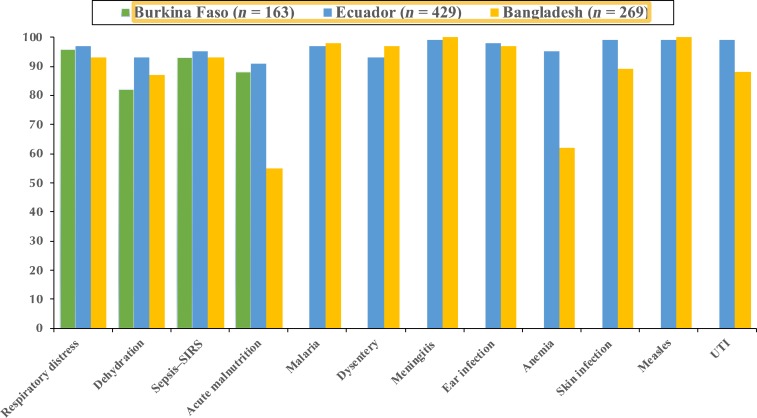
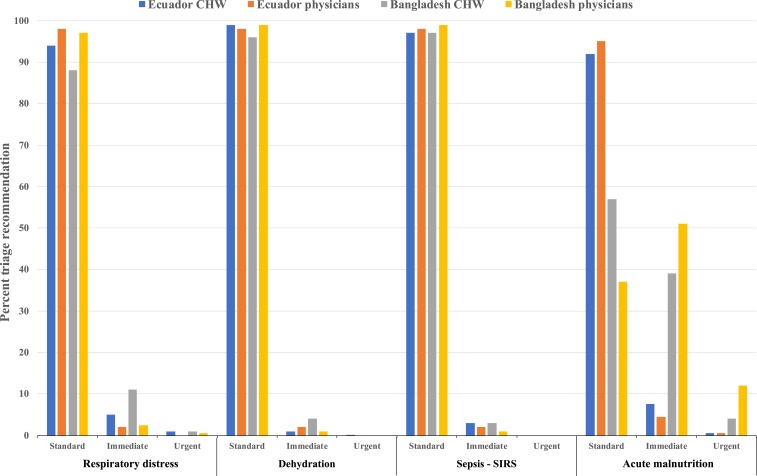
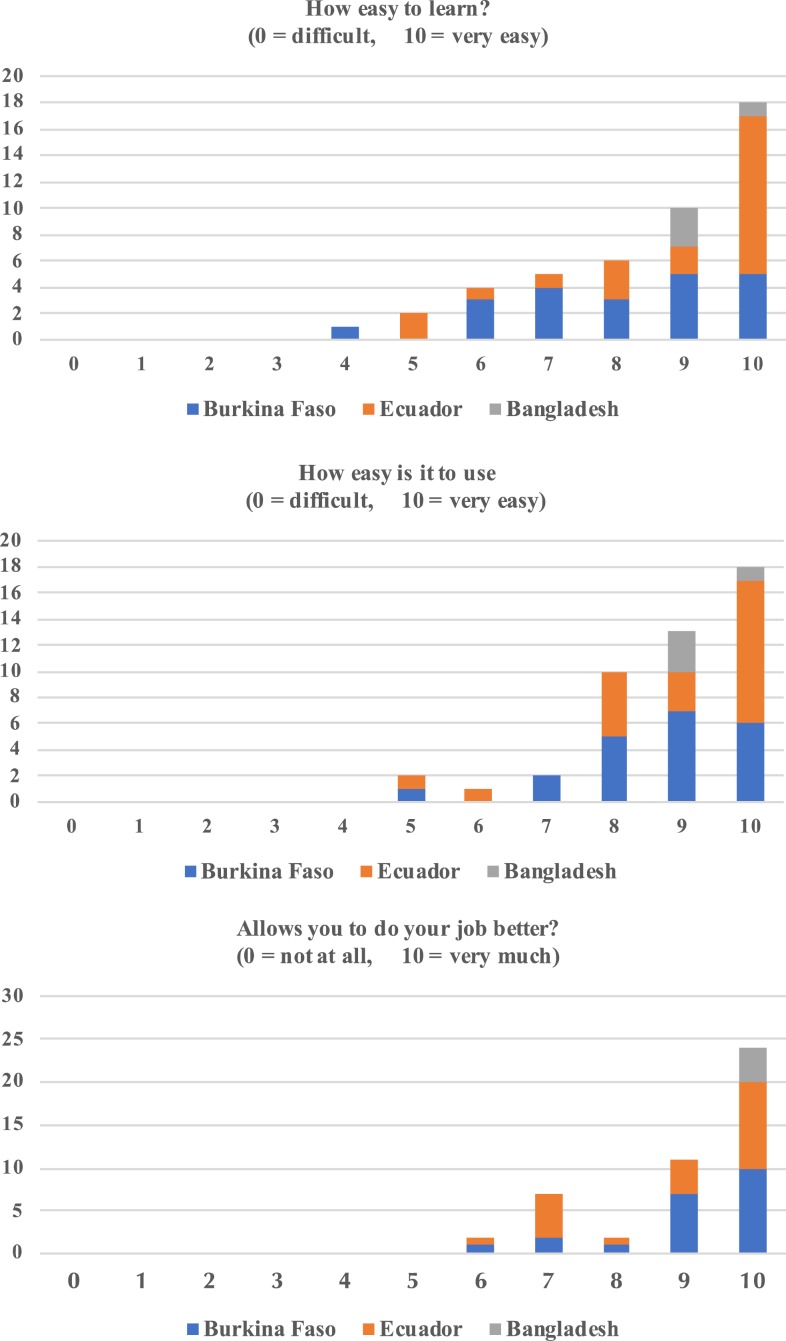
Approximately 3 million children younger than 5 years living in low- and middle-income countries (LMICs) die each year from treatable clinical conditions such as pneumonia, dehydration secondary to diarrhea, and malaria. A majority of these deaths could be prevented with early clinical assessments and appropriate therapeutic intervention. In this study, we describe the development and initial validation testing of a mobile health (mHealth) platform, MEDSINC®, designed for frontline health workers (FLWs) to perform clinical risk assessments of children aged 2-60 months. MEDSINC is a web browser-based clinical severity assessment, triage, treatment, and follow-up recommendation platform developed with physician-based Bayesian pattern recognition logic. Initial validation, usability, and acceptability testing were performed on 861 children aged between 2 and 60 months by 49 FLWs in Burkina Faso, Ecuador, and Bangladesh. MEDSINC-based clinical assessments by FLWs were independently and blindly correlated with clinical assessments by 22 local health-care professionals (LHPs). Results demonstrate that clinical assessments by FLWs using MEDSINC had a specificity correlation between 84% and 99% to LHPs, except for two outlier assessments (63% and 75%) at one study site, in which local survey prevalence data indicated that MEDSINC outperformed LHPs. In addition, MEDSINC triage recommendation distributions were highly correlated with those of LHPs, whereas usability and feasibility responses from LHP/FLW were collectively positive for ease of use, learning, and job performance. These results indicate that the MEDSINC platform could significantly increase pediatric health-care capacity in LMICs by improving FLWs' ability to accurately assess health status and triage of children, facilitating early life-saving therapeutic interventions.
Conflict of interest statement
Disclosure: B. A. F. and M. M. are employees of THINKMD, Inc. B. A. F. and B. H. are stock holders of THINKMD.
Figures
Comment in
-
Evidence and Transparency are Needed to Develop a Frontline Health Worker mHealth Assessment Platform.Am J Trop Med Hyg. 2019 Oct;101(4):948. doi: 10.4269/ajtmh.19-0411a. Am J Trop Med Hyg. 2019. PMID: 32519659 Free PMC article. No abstract available.
References
-
- UNICEF , 2015. Beyond averages-learning from the MDGs. Bucher K, Dooley T, Little C, Gonzalez Romo C, Sethna Z, Tamagni J, eds. Progress for Children. New York, NY: WHO.
-
- Watkins K. et al eds.; UNICEF , 2016. The State of the World’s Children 2106: A Fair Chance for Every Child. New York, NY: WHO.
-
- WHO , 2016. Global Strategy on Human Resources for Health: Workforce 2030. New York, NY: World Health Organization.
-
- Campbell J, Dussault G, Buchan J, Pozo-Martin F, Guerra Arias M, Leone C, Siyam A, Cometto G, eds.; WHO , 2014. A Universal Truth: No Health without a Workforce. New York, NY: World Health Organization.
