

Effectiveness and Acceptability of Cognitive Behavior Therapy Delivery Formats in Adults With Depression: A Network Meta-analysis
- PMID: 30994877
- PMCID: PMC6583673
- DOI: 10.1001/jamapsychiatry.2019.0268
Effectiveness and Acceptability of Cognitive Behavior Therapy Delivery Formats in Adults With Depression: A Network Meta-analysis
Erratum in
-
Error in Figure 3.JAMA Psychiatry. 2019 Sep 1;76(9):986. doi: 10.1001/jamapsychiatry.2019.2040. JAMA Psychiatry. 2019. PMID: 31314064 Free PMC article. No abstract available.
-
Error in Results and in the Figure 3B Label and Plotted Values.JAMA Psychiatry. 2022 Feb 1;79(2):180. doi: 10.1001/jamapsychiatry.2021.3357. JAMA Psychiatry. 2022. PMID: 34817574 Free PMC article. No abstract available.
Abstract
Importance: Cognitive behavior therapy (CBT) has been shown to be effective in the treatment of acute depression. However, whether CBT can be effectively delivered in individual, group, telephone-administered, guided self-help, and unguided self-help formats remains unclear.
Objective: To examine the most effective delivery format for CBT via a network meta-analysis.
Data sources: A database updated yearly from PubMed, PsycINFO, Embase, and the Cochrane Library. Literature search dates encompassed January 1, 1966, to January 1, 2018.
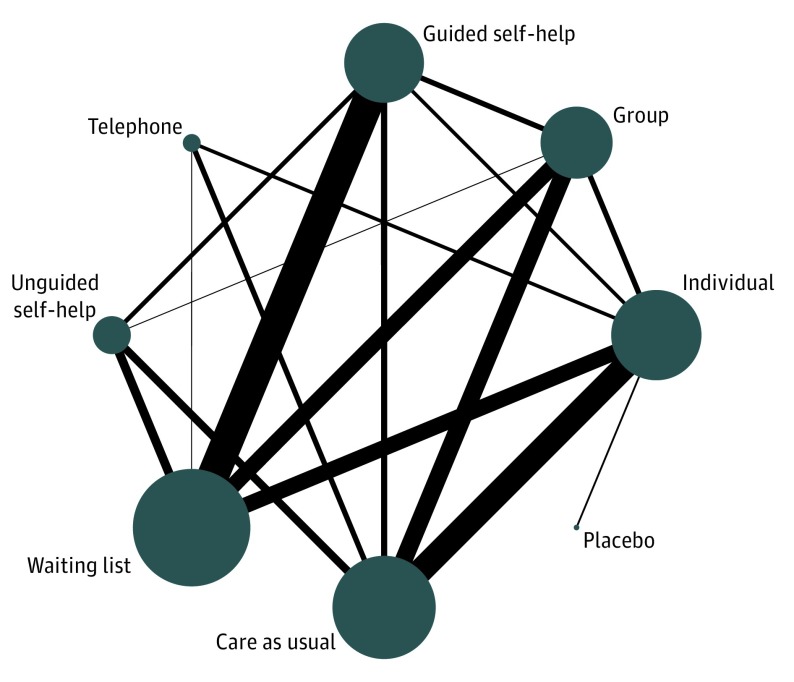
Study selection: Randomized clinical trials of CBT for adult depression. The 5 treatment formats were compared with each other and the control conditions (waiting list, care as usual, and pill placebo).
Data extraction and synthesis: PRISMA guidelines were used when extracting data and assessing data quality. Data were pooled using a random-effects model. Pairwise and network meta-analyses were conducted.
Main outcomes and measures: Severity of depression and acceptability of the treatment formats.
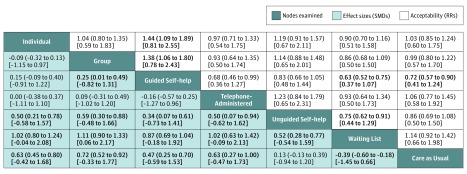
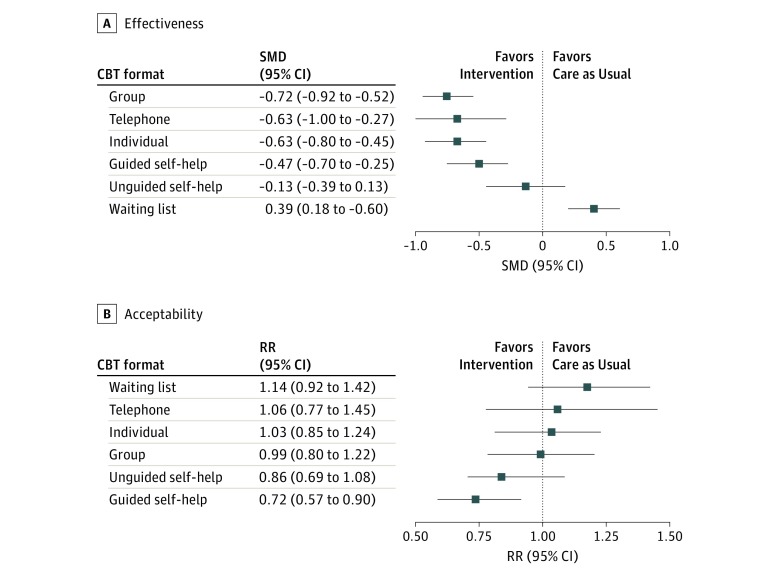
Results: A total of 155 trials with 15 191 participants compared 5 CBT delivery formats with 2 control conditions. In half of the studies (78 [50.3%]), patients met the criteria for a depressive disorder; in the other half (77 [49.7%]), participants scored above the cutoff point on a self-report measure. The effectiveness of individual, group, telephone, and guided self-help CBT did not differ statistically significantly from each other. These formats were statistically significantly more effective than the waiting list (standardized mean differences [SMDs], 0.87-1.02) and care as usual (SMDs, 0.47-0.72) control conditions as well as the unguided self-help CBT (SMDs, 0.34-0.59). In terms of acceptability (dropout for any reason), individual (relative risk [RR] = 1.44; 95% CI, 1.09-1.89) and group (RR = 1.38; 95% CI, 1.06-1.80) CBT were significantly better than guided self-help. Guided self-help was also less acceptable than being on a waiting list (RR = 0.63; 95% CI, 0.52-0.75) and care as usual (RR = 0.72; 95% CI, 0.57-0.90). Sensitivity analyses supported the overall findings.
Conclusions and relevance: For acute symptoms of depression, group, telephone, and guided self-help treatment formats appeared to be effective interventions, which may be considered as alternatives to individual CBT; although there were few indications of significant differences in efficacy between treatments with human support, guided self-help CBT may be less acceptable for patients than individual, group, or telephone formats.
Conflict of interest statement
Figures
Comment in
-
Can Network Meta-analysis Substitute for Direct Comparisons in Psychotherapy Trials?JAMA Psychiatry. 2019 Jul 1;76(7):678-679. doi: 10.1001/jamapsychiatry.2019.0243. JAMA Psychiatry. 2019. PMID: 30994866 No abstract available.
-
Errors in Relative Risks Reported in Figure 3 in a Network Meta-analysis of Cognitive Behavior Therapy Delivery Formats in Adults With Depression.JAMA Psychiatry. 2022 Feb 1;79(2):180. doi: 10.1001/jamapsychiatry.2021.3491. JAMA Psychiatry. 2022. PMID: 34817535 No abstract available.
References
-
- Beck AT, Rush AJ, Shaw BF, Emery G. Cognitive Therapy of Depression. New York, NY: The Guilford Press; 1979.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
