

The Diagnosis of Bronchopulmonary Dysplasia in Very Preterm Infants. An Evidence-based Approach
- PMID: 30995069
- PMCID: PMC6775872
- DOI: 10.1164/rccm.201812-2348OC
The Diagnosis of Bronchopulmonary Dysplasia in Very Preterm Infants. An Evidence-based Approach
Abstract
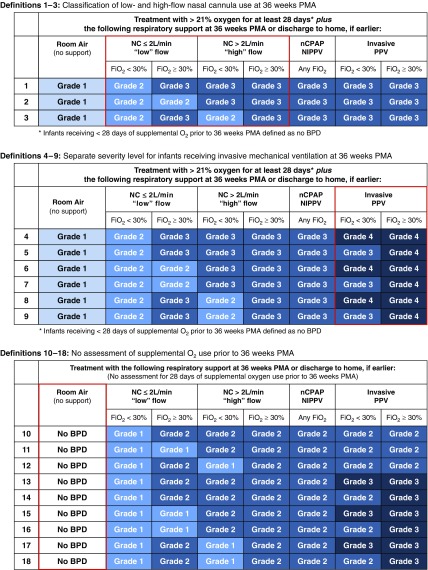
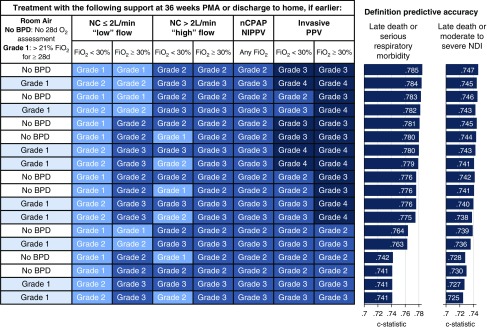
Rationale: Current diagnostic criteria for bronchopulmonary dysplasia rely heavily on the level and duration of oxygen therapy, do not reflect contemporary neonatal care, and do not adequately predict childhood morbidity.Objectives: To determine which of 18 prespecified, revised definitions of bronchopulmonary dysplasia that variably define disease severity according to the level of respiratory support and supplemental oxygen administered at 36 weeks' postmenstrual age best predicts death or serious respiratory morbidity through 18-26 months' corrected age.Methods: We assessed infants born at less than 32 weeks of gestation between 2011 and 2015 at 18 centers of the Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network.Measurements and Main Results: Of 2,677 infants, 683 (26%) died or developed serious respiratory morbidity. The diagnostic criteria that best predicted this outcome defined bronchopulmonary dysplasia according to treatment with the following support at 36 weeks' postmenstrual age, regardless of prior or current oxygen therapy: no bronchopulmonary dysplasia, no support (n = 773); grade 1, nasal cannula ≤2 L/min (n = 1,038); grade 2, nasal cannula >2 L/min or noninvasive positive airway pressure (n = 617); and grade 3, invasive mechanical ventilation (n = 249). These criteria correctly predicted death or serious respiratory morbidity in 81% of study infants. Rates of this outcome increased stepwise from 10% among infants without bronchopulmonary dysplasia to 77% among those with grade 3 disease. A similar gradient (33-79%) was observed for death or neurodevelopmental impairment.Conclusions: The definition of bronchopulmonary dysplasia that best predicted early childhood morbidity categorized disease severity according to the mode of respiratory support administered at 36 weeks' postmenstrual age, regardless of supplemental oxygen use.
Keywords: infant chronic lung disease; mechanical ventilation; supplemental oxygen.
Figures
Comment in
-
Bronchopulmonary Dysplasia: A Continuum of Lung Disease from the Fetus to the Adult.Am J Respir Crit Care Med. 2019 Sep 15;200(6):659-660. doi: 10.1164/rccm.201904-0875ED. Am J Respir Crit Care Med. 2019. PMID: 31091958 Free PMC article. No abstract available.
-
Reply to Bancalari et al. and to Isayama and Shah.Am J Respir Crit Care Med. 2019 Nov 15;200(10):1324-1325. doi: 10.1164/rccm.201906-1233LE. Am J Respir Crit Care Med. 2019. PMID: 31322416 Free PMC article. No abstract available.
-
Need for an International Consensus on the Definition of Bronchopulmonary Dysplasia.Am J Respir Crit Care Med. 2019 Nov 15;200(10):1323-1324. doi: 10.1164/rccm.201906-1127LE. Am J Respir Crit Care Med. 2019. PMID: 31322422 Free PMC article. No abstract available.
-
Diagnostic Classification of Bronchopulmonary Dysplasia: A Compromise between Defining Lung Disease versus Long-Term Outcome Prediction.Am J Respir Crit Care Med. 2019 Nov 15;200(10):1322-1323. doi: 10.1164/rccm.201906-1130LE. Am J Respir Crit Care Med. 2019. PMID: 31322424 Free PMC article. No abstract available.
-
The diagnosis of bronchopulmonary dysplasia in very preterm infants-Which is the better definition?Acta Paediatr. 2021 Feb;110(2):720-721. doi: 10.1111/apa.15624. Epub 2020 Nov 21. Acta Paediatr. 2021. PMID: 33222304 No abstract available.
References
-
- Stoll BJ, Hansen NI, Bell EF, Walsh MC, Carlo WA, Shankaran S, et al. Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993-2012. JAMA. 2015;314:1039–1051. - PMC - PubMed
-
- Ehrenkranz RA, Walsh MC, Vohr BR, Jobe AH, Wright LL, Fanaroff AA, et al. National Institute of Child Health and Human Development Neonatal Research Network. Validation of the National Institutes of Health consensus definition of bronchopulmonary dysplasia. Pediatrics. 2005;116:1353–1360. - PubMed
-
- Schmidt B, Roberts RS, Davis PG, Doyle LW, Asztalos EV, Opie G, et al. Caffeine for Apnea of Prematurity (CAP) Trial Investigators; Caffeine for Apnea of Prematurity CAP Trial Investigators. Prediction of late death or disability at age 5 years using a count of 3 neonatal morbidities in very low birth weight infants. J Pediatr. 2015;167:982–986.e2. - PubMed
-
- Álvarez-Fuente M, Arruza L, Muro M, Zozaya C, Avila A, López-Ortego P, et al. The economic impact of prematurity and bronchopulmonary dysplasia. Eur J Pediatr. 2017;176:1587–1593. - PubMed
-
- Poets CF, Lorenz L. Prevention of bronchopulmonary dysplasia in extremely low gestational age neonates: current evidence. Arch Dis Child Fetal Neonatal Ed. 2018;103:F285–F291. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
