

Zika viruses of African and Asian lineages cause fetal harm in a mouse model of vertical transmission
- PMID: 30995223
- PMCID: PMC6488094
- DOI: 10.1371/journal.pntd.0007343
Zika viruses of African and Asian lineages cause fetal harm in a mouse model of vertical transmission
Abstract
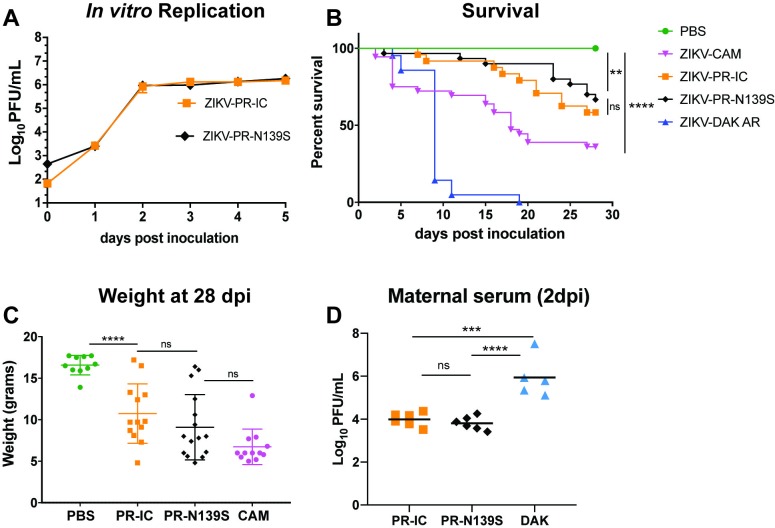
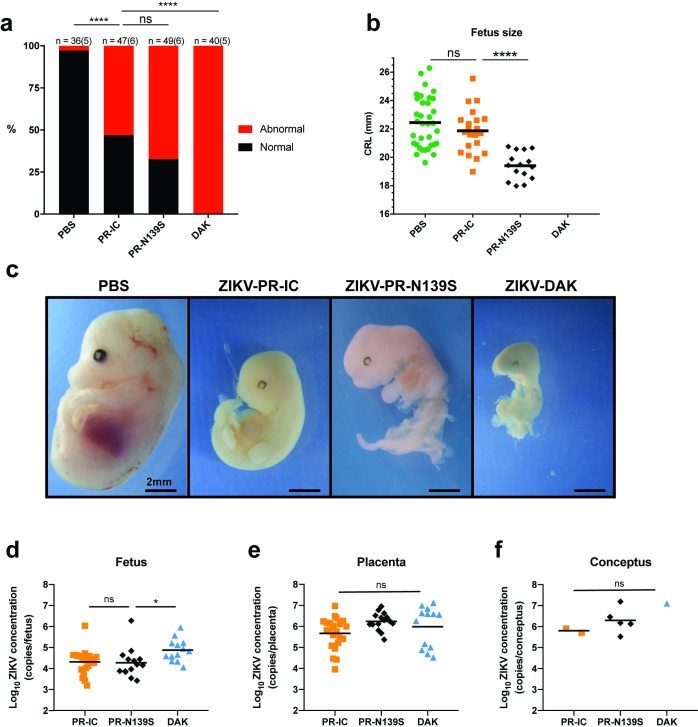
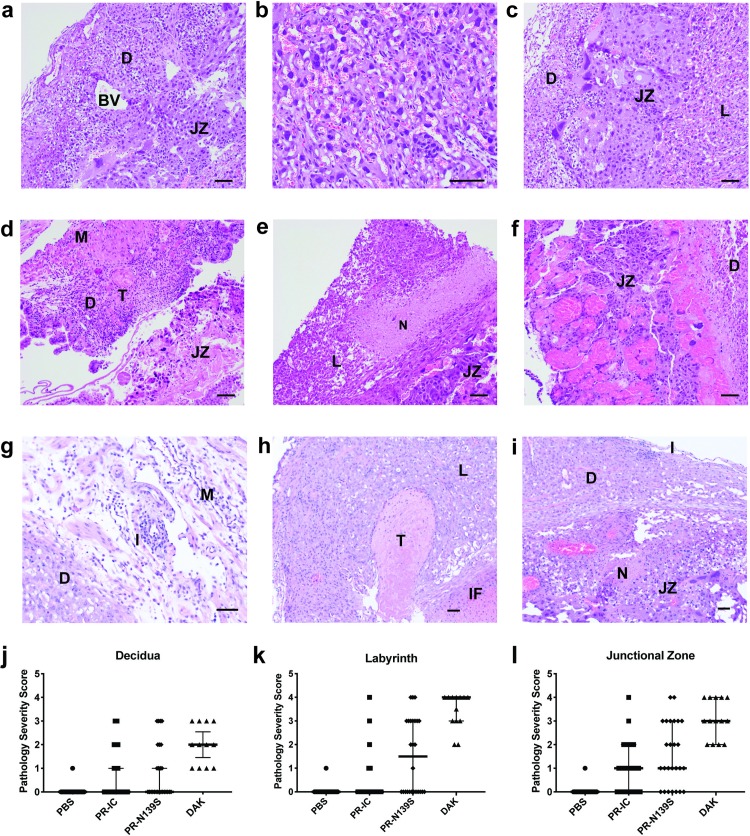
Congenital Zika virus (ZIKV) infection was first linked to birth defects during the American outbreak in 2015/2016. It has been proposed that mutations unique to the Asian/American-genotype explain, at least in part, the ability of Asian/American ZIKV to cause congenital Zika syndrome (CZS). Recent studies identified mutations in ZIKV infecting humans that arose coincident with the outbreak in French Polynesia and were stably maintained during subsequent spread to the Americas. Here we show that African ZIKV can infect and harm fetuses and that the S139N substitution that has been associated with the American outbreak is not essential for fetal harm. Our findings, in a vertical transmission mouse model, suggest that ZIKV will remain a threat to pregnant women for the foreseeable future, including in Africa, Southeast Asia, and the Americas. Additional research is needed to better understand the risks associated with ZIKV infection during pregnancy, both in areas where the virus is newly endemic and where it has been circulating for decades.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
African-Lineage Zika Virus Replication Dynamics and Maternal-Fetal Interface Infection in Pregnant Rhesus Macaques.J Virol. 2021 Jul 26;95(16):e0222020. doi: 10.1128/JVI.02220-20. Epub 2021 Jul 26. J Virol. 2021. PMID: 34076485 Free PMC article.
-
Neutralizing human antibodies prevent Zika virus replication and fetal disease in mice.Nature. 2016 Dec 15;540(7633):443-447. doi: 10.1038/nature20564. Epub 2016 Nov 7. Nature. 2016. PMID: 27819683 Free PMC article.
-
Epidemic Zika virus strains from the Asian lineage induce an attenuated fetal brain pathogenicity.Nat Commun. 2024 Dec 30;15(1):10870. doi: 10.1038/s41467-024-55155-4. Nat Commun. 2024. PMID: 39738084 Free PMC article.
-
Epidemiology of Zika Virus Infection.J Infect Dis. 2017 Dec 16;216(suppl_10):S868-S874. doi: 10.1093/infdis/jix434. J Infect Dis. 2017. PMID: 29267914 Free PMC article. Review.
-
Congenital Abnormalities: Consequence of Maternal Zika Virus Infection: A Narrative Review.Infect Disord Drug Targets. 2017;17(1):3-13. doi: 10.2174/1871526516666161018104916. Infect Disord Drug Targets. 2017. PMID: 27758685 Review.
Cited by
-
Genetic Diversity of Collaborative Cross Mice Controls Viral Replication, Clinical Severity, and Brain Pathology Induced by Zika Virus Infection, Independently of Oas1b.J Virol. 2020 Jan 17;94(3):e01034-19. doi: 10.1128/JVI.01034-19. Print 2020 Jan 17. J Virol. 2020. PMID: 31694939 Free PMC article.
-
Recent African strains of Zika virus display higher transmissibility and fetal pathogenicity than Asian strains.Nat Commun. 2021 Feb 10;12(1):916. doi: 10.1038/s41467-021-21199-z. Nat Commun. 2021. PMID: 33568638 Free PMC article.
-
From Mosquito Bites to Sexual Transmission: Evaluating Mouse Models of Zika Virus Infection.Viruses. 2021 Nov 8;13(11):2244. doi: 10.3390/v13112244. Viruses. 2021. PMID: 34835050 Free PMC article. Review.
-
Zika structural genes determine the virulence of African and Asian lineages.Emerg Microbes Infect. 2020 Dec;9(1):1023-1033. doi: 10.1080/22221751.2020.1753583. Emerg Microbes Infect. 2020. PMID: 32419649 Free PMC article.
-
Primary infection with Zika virus provides one-way heterologous protection against Spondweni virus infection in rhesus macaques.Sci Adv. 2023 Jun 30;9(26):eadg3444. doi: 10.1126/sciadv.adg3444. Epub 2023 Jun 30. Sci Adv. 2023. PMID: 37390207 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
