

Hepatorenal Syndrome
- PMID: 30996046
- PMCID: PMC6500947
- DOI: 10.2215/CJN.12451018
Hepatorenal Syndrome
Abstract
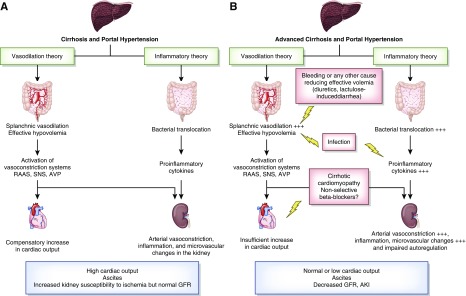
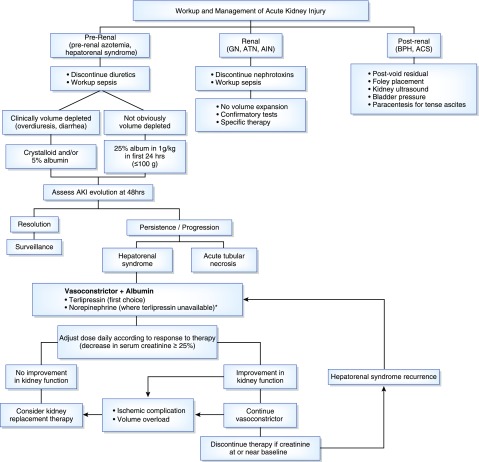
Hepatorenal syndrome is a severe complication of end-stage cirrhosis characterized by increased splanchnic blood flow, hyperdynamic state, a state of decreased central volume, activation of vasoconstrictor systems, and extreme kidney vasoconstriction leading to decreased GFR. The contribution of systemic inflammation, a key feature of cirrhosis, in the development of hepatorenal syndrome has been highlighted in recent years. The mechanisms by which systemic inflammation precipitates kidney circulatory changes during hepatorenal syndrome need to be clarified. Early diagnosis is central in the management and recent changes in the definition of hepatorenal syndrome help identify patients at an earlier stage. Vasoconstrictive agents (terlipressin in particular) and albumin are the first-line treatment option. Several controlled studies proved that terlipressin is effective at reversing hepatorenal syndrome and may improve short-term survival. Not all patients are responders, and even in responders, early mortality rates are very high in the absence of liver transplantation. Liver transplantation is the only curative treatment of hepatorenal syndrome. In the long term, patients transplanted with hepatorenal syndrome tend to have lower GFR compared with patients without hepatorenal syndrome. Differentiating hepatorenal syndrome from acute tubular necrosis (ATN) is often a challenging yet important step because vasoconstrictors are not justified for the treatment of ATN. Hepatorenal syndrome and ATN may be considered as a continuum rather than distinct entities. Emerging biomarkers may help differentiate these two conditions and provide prognostic information on kidney recovery after liver transplantation, and potentially affect the decision for simultaneous liver-kidney transplantation.
Keywords: Albumins; Biomarkers; Early Diagnosis; Hepatorenal Syndrome; Inflammation; Kidney Tubular Necrosis, Acute; Liver Cirrhosis; Liver Transplantation; Lypressin; Prognosis; Renal Circulation; Vasoconstriction; Vasoconstrictor Agents; acute kidney injury; glomerular filtration rate; hepatorenal; kidney transplantation; liver transplantation; terlipressin.
Copyright © 2019 by the American Society of Nephrology.
Figures
References
-
- Rice JB, White AG, Galebach P, Korenblat KM, Wagh A, Lovelace B, Wan GJ, Jamil K: The burden of hepatorenal syndrome among commercially insured and Medicare patients in the United States. Curr Med Res Opin 33: 1473–1480, 2017 - PubMed
-
- Angeli P, Gines P, Wong F, Bernardi M, Boyer TD, Gerbes A, Moreau R, Jalan R, Sarin SK, Piano S, Moore K, Lee SS, Durand F, Salerno F, Caraceni P, Kim WR, Arroyo V, Garcia-Tsao G; International Club of Ascites: Diagnosis and management of acute kidney injury in patients with cirrhosis: Revised consensus recommendations of the International Club of Ascites. Gut 64: 531–537, 2015 - PubMed
-
- Amathieu R, Al-Khafaji A, Sileanu FE, Foldes E, DeSensi R, Hilmi I, Kellum JA: Significance of oliguria in critically ill patients with chronic liver disease. Hepatology 66: 1592–1600, 2017 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
