

Endoscopic Ultrasound-guided Drainage of a Mediastinal Abscess Caused by an Ingested Fish Bone
- PMID: 30996160
- PMCID: PMC6709328
- DOI: 10.2169/internalmedicine.1992-18
Endoscopic Ultrasound-guided Drainage of a Mediastinal Abscess Caused by an Ingested Fish Bone
Abstract
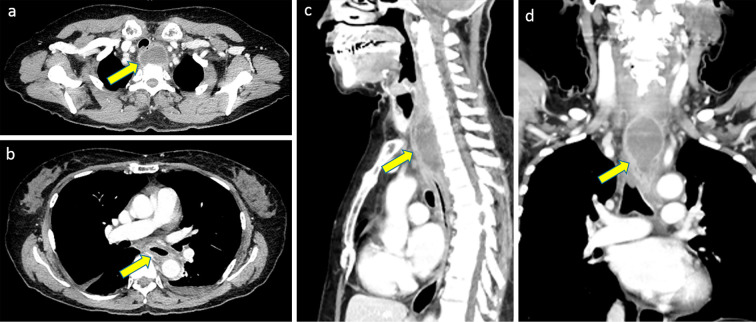
Cases of foreign body ingestion are encountered relatively often in clinical settings; however, serious complications are rare. In such cases, mediastinal abscess due to esophageal perforation can become a life-threatening complication. Although highly invasive, surgery is often used as the first-line treatment. We herein report the case of a 65-year-old woman who presented with complaints of progressive odynophagia and dysphagia for 2 weeks following a fish meal. Enhanced cervicothoracic computed tomography demonstrated an enhanced round mass with peripheral contrasted margins. The mass was diagnosed as a mediastinal abscess resulting from esophageal perforation caused by a fish bone. Endoscopic ultrasound-guided abscess drainage (EUS-AD) was performed using a nasobiliary drainage tube (NDT). Two weeks later, the abscess had completely disappeared. EUS-AD was safe and effective in this case; furthermore, external drainage using NDT was suitable for this abscess located very close to the upper esophageal sphincter.
Keywords: endoscopic ultrasound-guided abscess drainage; fish bone; mediastinal abscess.
Conflict of interest statement
Figures



References
-
- Eisen GM, Baron TH, Dominitz JA, et al. . Guideline for the management of ingested foreign bodies. Gastrointest Endosc 55: 802-806, 2002. - PubMed
-
- Sung SH, Jeon SW, Son HS, et al. . Factors predictive of risk for complications in patients with esophageal foreign bodies. Dig Liver Dis 43: 632-635, 2011. - PubMed
-
- Grodinsky M, Holyoke EA. The fasciae and fascial spaces of the head, neck and adjacent regions. Am J Anat 63: 367-408, 1938.
-
- Ahmad R, Ishlah W, Shaharudin MH, et al. . Posterior mediastinal abscess secondary to esophageal perforation following fish bone ingestion. Med J Malaysia 63: 162-163, 2008. - PubMed