

A 29-year-old Woman with Recurrent Pregnancy-induced Hypertension Based on Vascular Compression of the Medulla Oblongata
- PMID: 30996172
- PMCID: PMC6709317
- DOI: 10.2169/internalmedicine.2382-18
A 29-year-old Woman with Recurrent Pregnancy-induced Hypertension Based on Vascular Compression of the Medulla Oblongata
Abstract
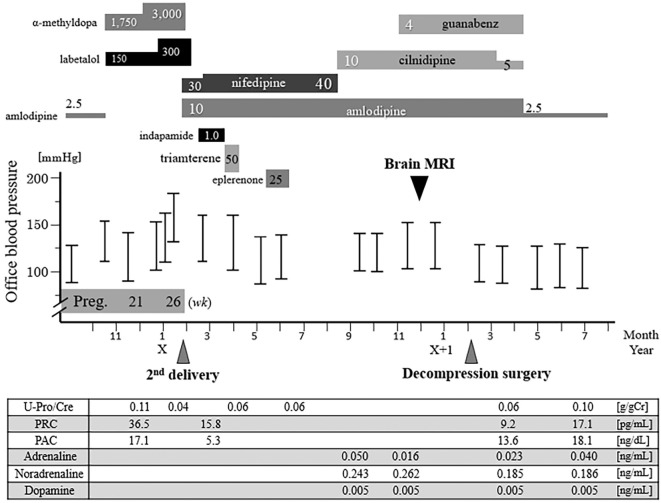
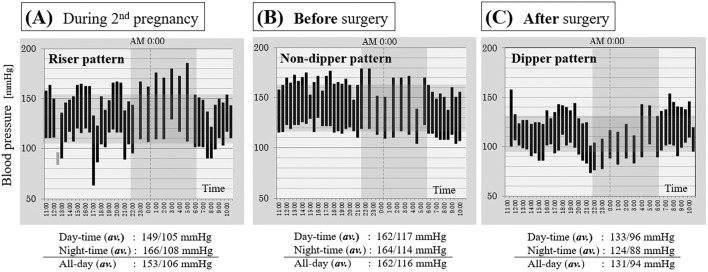
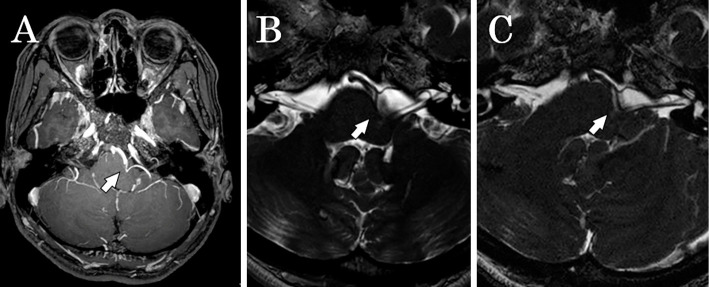
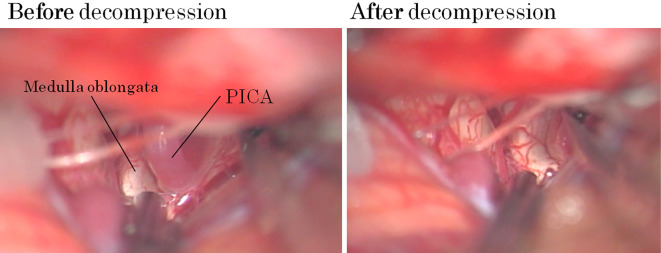
We present a report of a 29-year-old woman with non-dipper type refractory hypertension due to the vascular compression of the medulla oblongata. The patient was diagnosed with hypertension at 17 years of age and underwent emergency Caesarean section at 26 weeks of gestation during 2 pregnancies due to severe high blood pressure. We suspected medullary compression by the curved posterior inferior cerebellar artery as the cause of her intractable hypertension, and she underwent Jannetta's decompression surgery. After the surgery, her blood pressure swiftly decreased to almost within the normal range, and her blood pressure pattern normalized to dipper type.
Keywords: Jannetta's decompression surgery; intractable hypertension; medullary compression; non-dipper type; pregnancy-induced hypertension.
Conflict of interest statement
Figures
Similar articles
-
Microvascular decompression of the left lateral medulla oblongata for severe refractory neurogenic hypertension.Neurosurgery. 1998 Jul;43(1):1-6; discussion 6-9. doi: 10.1097/00006123-199807000-00001. Neurosurgery. 1998. PMID: 9657182
-
Medullary Compression Due to Ectatic Vertebral Artery-Case Report and Review of Literature.J Stroke Cerebrovasc Dis. 2020 Jan;29(1):104460. doi: 10.1016/j.jstrokecerebrovasdis.2019.104460. Epub 2019 Nov 4. J Stroke Cerebrovasc Dis. 2020. PMID: 31699578 Review.
-
[Neurovascular compression of the medulla oblongata: a rare cause of secondary hypertension].Orv Hetil. 2014 May 25;155(21):838-42. doi: 10.1556/OH.2014.29908. Orv Hetil. 2014. PMID: 24836320 Hungarian.
-
[A case report of hemiparesis due to compression of the medulla oblongata by an elongated vertebral artery].No Shinkei Geka. 2001 Mar;29(3):247-51. No Shinkei Geka. 2001. PMID: 11321794 Japanese.
-
Successful Treatment with Microvascular Decompression Surgery of a Patient with Hemiparesis Caused by Vertebral Artery Compression of the Medulla Oblongata: Case Report and Review of the Literature.World Neurosurg. 2017 Dec;108:994.e11-994.e19. doi: 10.1016/j.wneu.2017.09.016. Epub 2017 Sep 9. World Neurosurg. 2017. PMID: 28899835 Review.
Cited by
-
Vertebral artery compression of the medulla oblongata: A benign radiological finding?Surg Neurol Int. 2022 Feb 4;13:36. doi: 10.25259/SNI_1161_2021. eCollection 2022. Surg Neurol Int. 2022. PMID: 35242402 Free PMC article.
-
Lateral medullary vascular compression manifesting as paroxysmal hypertension.Acta Neurochir (Wien). 2024 Mar 15;166(1):139. doi: 10.1007/s00701-024-06032-y. Acta Neurochir (Wien). 2024. PMID: 38488893 Free PMC article.
References
-
- Vongpatanasin W. Resistant hypertension: a review of diagnosis and management. JAMA 311: 2216-2224, 2014. - PubMed
-
- Boogaarts HD, Menovsky T, de Vries J, et al. . Primary hypertension and neurovascular compression: a meta-analysis of magnetic resonance imaging studies. J Neurosurg 116: 147-156, 2012. - PubMed