

Automated sleep stage classification based on tracheal body sound and actigraphy
- PMID: 30996721
- PMCID: PMC6449867
- DOI: 10.3205/000268
Automated sleep stage classification based on tracheal body sound and actigraphy
Abstract
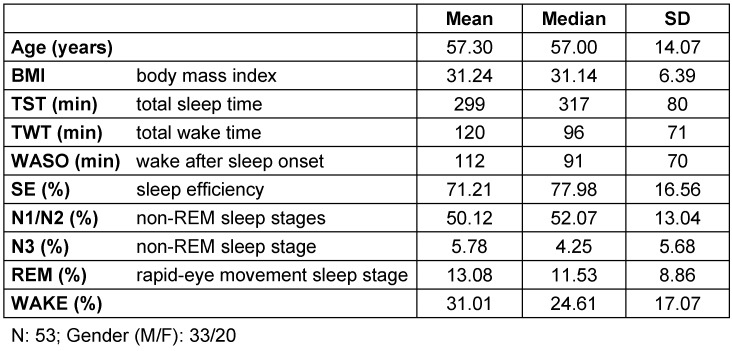
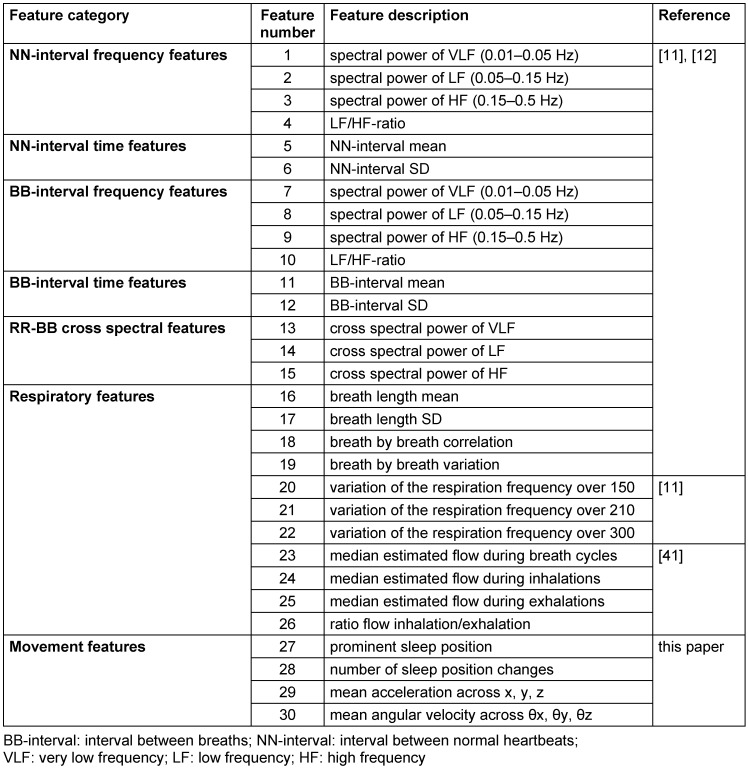
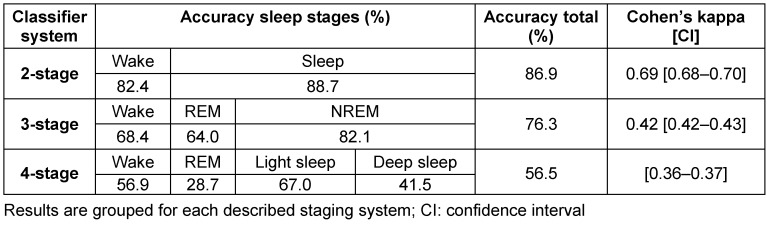
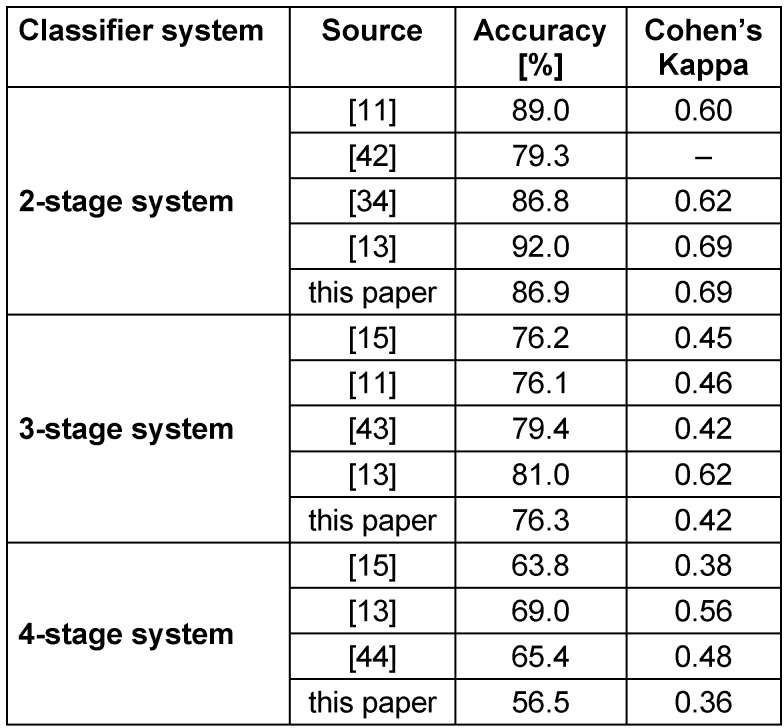
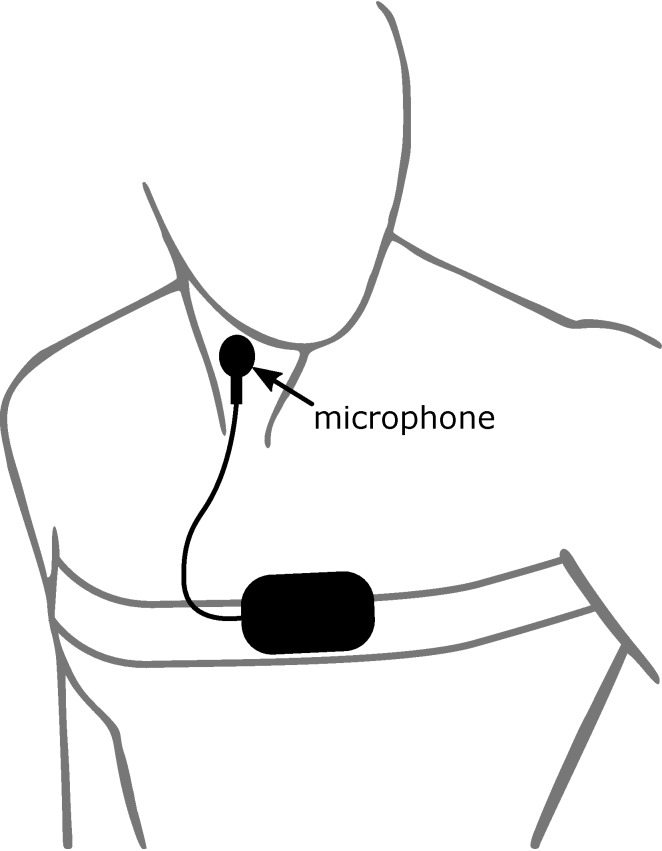
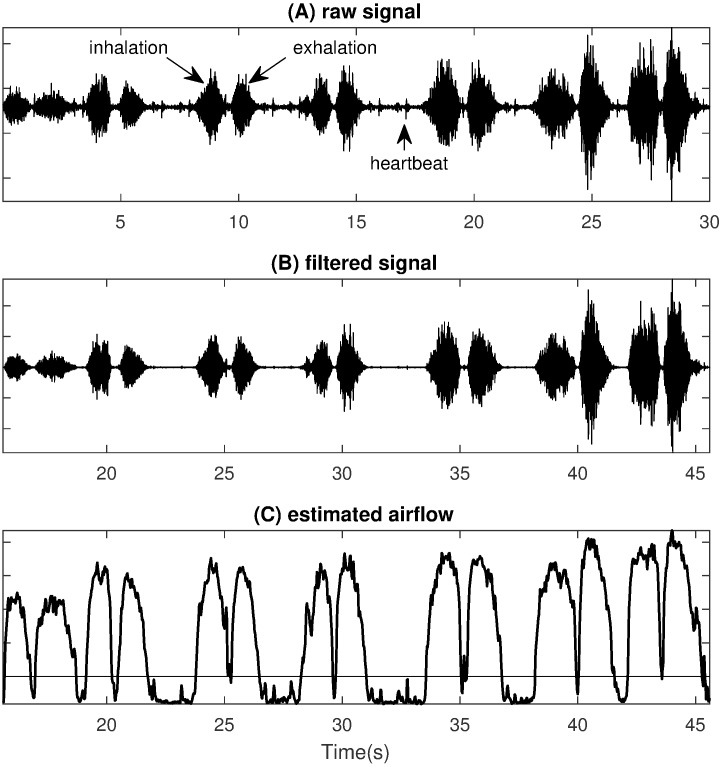
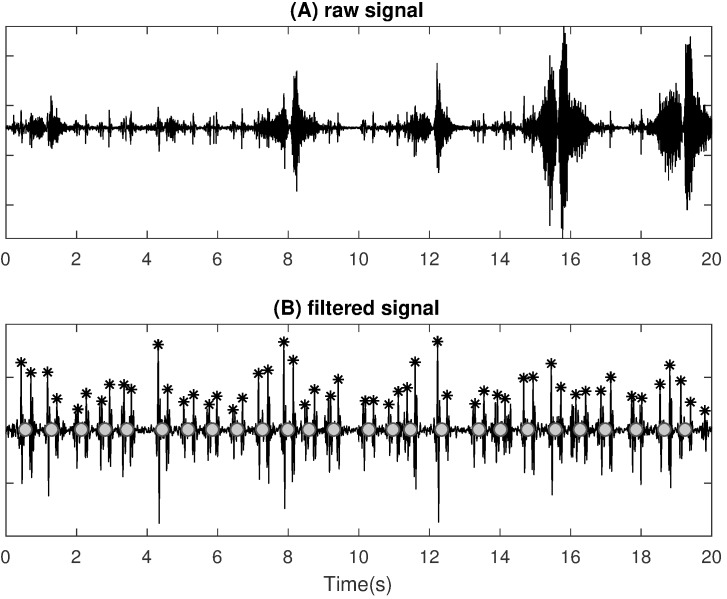
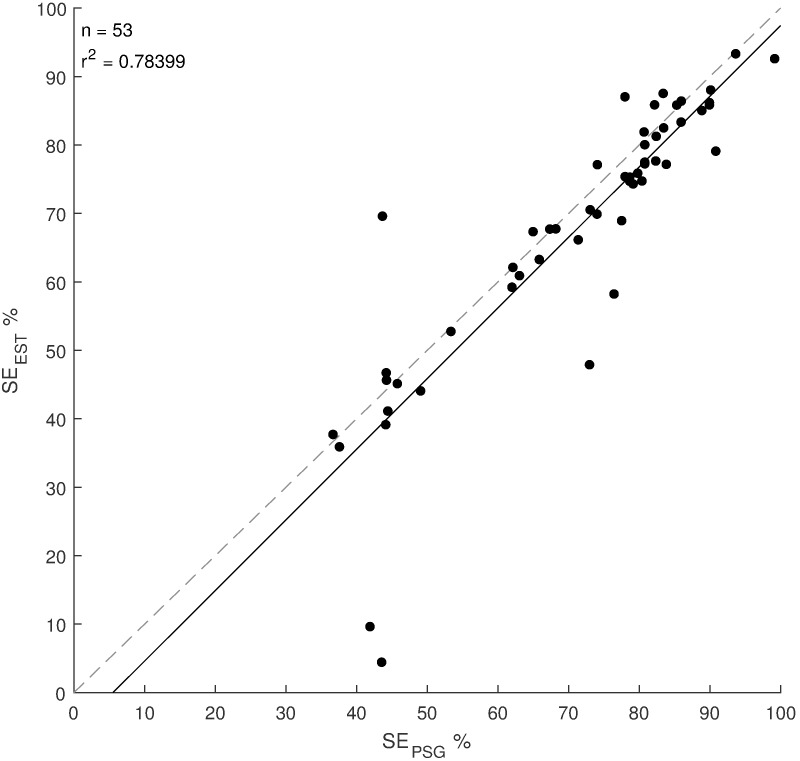
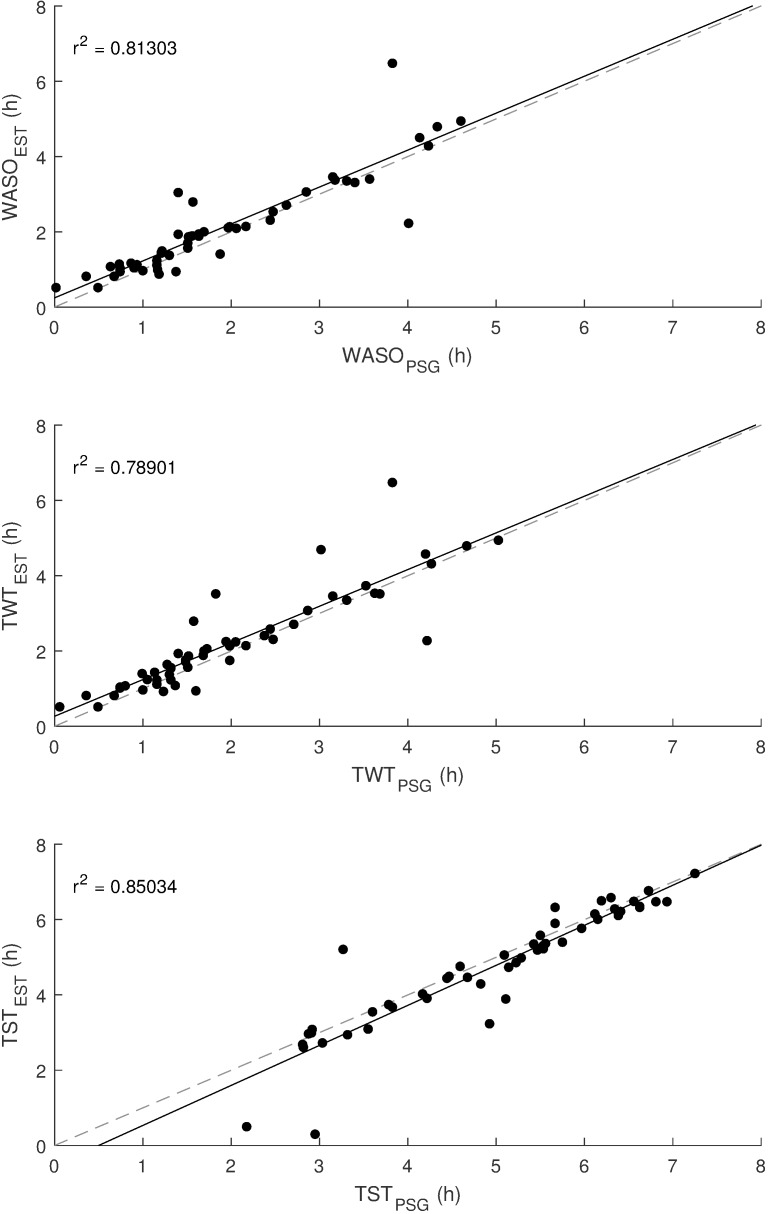
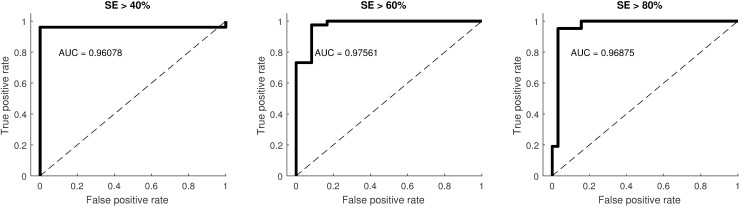
The current gold standard for assessment of most sleep disorders is the in-laboratory polysomnography (PSG). This approach produces high costs and inconveniences for the patients. An accessible and simple preliminary screening method to diagnose the most common sleep disorders and to decide whether a PSG is necessary or not is therefore desirable. A minimalistic type-4 monitoring system which utilized tracheal body sound and actigraphy to accurately diagnose the obstructive sleep apnea syndrome was previously developed. To further improve the diagnostic ability of said system, this study aims to examine if it is possible to perform automated sleep staging utilizing body sound to extract cardiorespiratory features and actigraphy to extract movement features. A linear discriminant classifier based on those features was used for automated sleep staging using the type-4 sleep monitor. For validation 53 subjects underwent a full-night screening at Ulm University Hospital using the developed sleep monitor in addition to polysomnography. To assess sleep stages from PSG, a trained technician manually evaluated EEG, EOG, and EMG recordings. The classifier reached 86.9% accuracy and a Kappa of 0.69 for sleep/wake classification, 76.3% accuracy and a Kappa of 0.42 for Wake/REM/NREM classification, and 56.5% accuracy and a Kappa of 0.36 for Wake/REM/light sleep/deep sleep classification. For the calculation of sleep efficiency (SE), a coefficient of determination r2 of 0.78 is reached. Additionally, subjects were classified into groups of SEs (SE≥40%, SE≥60% and SE≥80%). A Cohen's Kappa >0.61 was reached for all groups, which is considered as substantial agreement. The presented method provides satisfactory performance in sleep/wake and wake/REM/NREM sleep staging while maintaining a simple setup and offering high comfort. This minimalistic approach may address the need for a simple yet reliable preliminary sleep screening in an ambulatory setting.
Der aktuelle Goldstandard für die Beurteilung der meisten Schlafstörungen ist die Polysomnographie (PSG). Diese Methode der Diagnose ist mit hohen Kosten und Unannehmlichkeiten für die Patienten verbunden. Eine einfache Methode der Diagnose der häufigsten Schlafstörungen ist daher wünschenswert. Hierzu wurde ein minimalistischer Typ-4-Schlafmonitor, welcher Körperschall und Aktigraphie zur Diagnose des obstruktiven Schlafapnoe-Syndroms einsetzt, entwickelt. Um die Diagnosefähigkeit dieses Systems zu erweitern, soll in dieser Studie untersucht werden, ob der Schlafmonitor automatisiert Schlafstadien klassifizieren kann. Hierbei wird Körperschall verwendet, um kardiorespiratorische Merkmale zu extrahieren, und Aktigraphie, um Bewegungsmerkmale zu extrahieren.Ein auf diesen Merkmalen basierender linearer Diskriminanzklassifizierer wurde für die automatisierte Klassifizierung von Schlafstadien mit dem vorgestellten Typ-4-Schlafmonitor verwendet. Zur Validierung wurden 53 Probanden am Universitätsklinikum Ulm zusätzlich zur PSG einem nächtlichen Screening mit dem entwickelten Schlafmonitor unterzogen. Zur Beurteilung der Schlafstadien der PSG hat ein geschulter Techniker EEG-, EOG- und EMG-Aufnahmen manuell ausgewertet. Der Klassifikator erreichte eine Genauigkeit von 86,9% und ein Kappa von 0,69 für Schlaf/Wach-Klassifizierung, 76,3% Genauigkeit und ein Kappa von 0,42 für Wach/REM/NREM-Klassifizierung, und 56,5% Genauigkeit und ein Kappa von 0,36 für Wach/REM/Leichtschlaf/Tiefschlaf-Klassifizierung. Für die Berechnung der Schlafeffizienz (SE) wird ein Bestimmtheitsmaß r2 von 0,78 erreicht. Zusätzlich wurden die Probanden in Gruppen von SEs eingeteilt (SE≥40%, SE≥60% und SE≥80%). Ein Cohen’s Kappa >0,61 wurde für alle Gruppen erreicht, was als substantielle Übereinstimmung angesehen wird.Die vorgestellte Methode bietet eine zufriedenstellende Leistung in der Schlaf/Wach- und Wach/REM/NREM-Schlaf-Klassifizierung bei einfachem Aufbau und hohem Patientenkomfort. Dieser minimalistische Ansatz kann den Bedarf an einem einfachen aber zuverlässigen Vorab-Schlaf-Screening im ambulanten Bereich abdecken.
Keywords: monitoring; movement analysis; respiratory sounds; sleep staging.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Validation of a New System Using Tracheal Body Sound and Movement Data for Automated Apnea-Hypopnea Index Estimation.J Clin Sleep Med. 2017 Oct 15;13(10):1123-1130. doi: 10.5664/jcsm.6752. J Clin Sleep Med. 2017. PMID: 28859722 Free PMC article.
-
Validation of Photoplethysmography-Based Sleep Staging Compared With Polysomnography in Healthy Middle-Aged Adults.Sleep. 2017 Jul 1;40(7). doi: 10.1093/sleep/zsx097. Sleep. 2017. PMID: 28838130
-
Sleep staging based on autonomic signals: a multi-center validation study.J Clin Sleep Med. 2011 Jun 15;7(3):301-6. doi: 10.5664/JCSM.1078. J Clin Sleep Med. 2011. PMID: 21677901 Free PMC article.
-
Monitoring healthy and disturbed sleep through smartphone applications: a review of experimental evidence.Sleep Breath. 2019 Mar;23(1):13-24. doi: 10.1007/s11325-018-1661-3. Epub 2018 Apr 23. Sleep Breath. 2019. PMID: 29687190 Review.
-
Polysomnography.Handb Clin Neurol. 2019;160:381-392. doi: 10.1016/B978-0-444-64032-1.00025-4. Handb Clin Neurol. 2019. PMID: 31277862 Review.
Cited by
-
Complexity of Body Movements during Sleep in Children with Autism Spectrum Disorder.Entropy (Basel). 2021 Mar 31;23(4):418. doi: 10.3390/e23040418. Entropy (Basel). 2021. PMID: 33807381 Free PMC article.
-
End-to-End Sleep Staging Using Nocturnal Sounds from Microphone Chips for Mobile Devices.Nat Sci Sleep. 2022 Jun 25;14:1187-1201. doi: 10.2147/NSS.S361270. eCollection 2022. Nat Sci Sleep. 2022. PMID: 35783665 Free PMC article.
-
Sleep/Wakefulness Detection Using Tracheal Sounds and Movements.Nat Sci Sleep. 2020 Nov 17;12:1009-1021. doi: 10.2147/NSS.S276107. eCollection 2020. Nat Sci Sleep. 2020. PMID: 33235534 Free PMC article.
-
Alternatives to Polysomnography for the Diagnosis of Pediatric Obstructive Sleep Apnea.Diagnostics (Basel). 2023 Jun 3;13(11):1956. doi: 10.3390/diagnostics13111956. Diagnostics (Basel). 2023. PMID: 37296808 Free PMC article. Review.
-
A Systematic Review of Sensing Technologies for Wearable Sleep Staging.Sensors (Basel). 2021 Feb 24;21(5):1562. doi: 10.3390/s21051562. Sensors (Basel). 2021. PMID: 33668118 Free PMC article.
References
-
- Cappuccio FP, Miller MA, Lockley SW, editors. Sleep, health, and society. Oxford: Oxford Univ. Press; 2010.
-
- Penzel T, Blau A, Garcia C, Schöbel C, Sebert M, Fietze I. Portable monitoring in sleep apnea. Curr Respir Care Rep. 2012;1(2):139–145. doi: 10.1007/s13665-012-0014-0. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
