

Contribution of adverse events to death of hospitalised patients
- PMID: 30997413
- PMCID: PMC6440591
- DOI: 10.1136/bmjoq-2018-000377
Contribution of adverse events to death of hospitalised patients
Abstract
Background: There is no standardised method to investigate death as a patient safety indicator and we need valid and reliable measurements to use adverse events contributing to death as a quality measure.
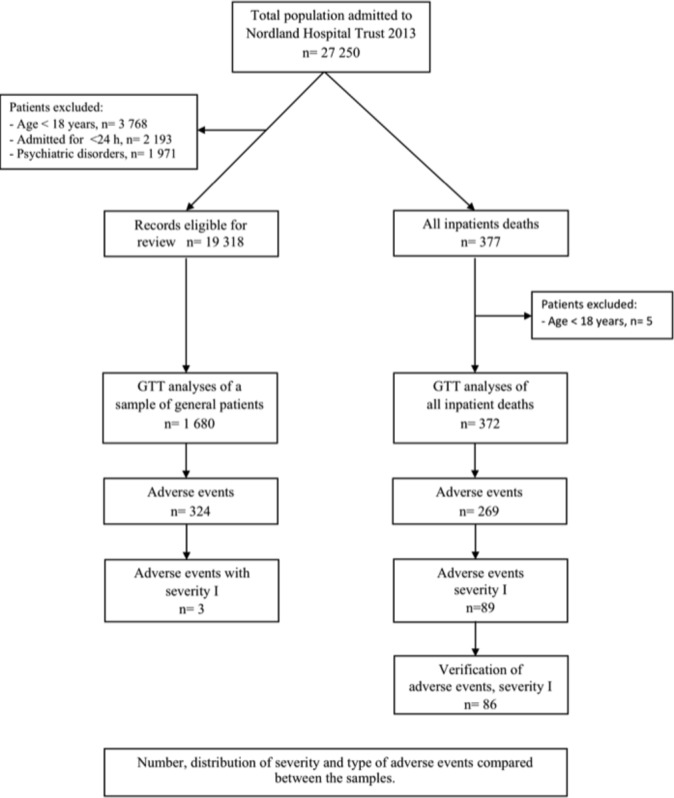
Objective: To investigate the contribution of severe adverse events to death in hospitalised patients and clarify methodological differences using the Global Trigger Tool method on all inpatient deaths compared with a sample of general hospitalised patients.
Method: Retrospective records reviewing using the Global Trigger Tool method.
Results: In 0.3% of hospital admissions, adverse events contribute to inpatient death. Patients who die in hospital have twice the rate of adverse events per 1000 patient days compared with general patients, 76.7 vs 36.5 (p<0.001, RR 2.10, 95% CI 1.79 to 2.47). Patients dying in hospital experience seven times the rate of severe adverse events, 38.4% vs 5.2% (p<0.001, RR 2.10, 95% CI 1.79 to 2.47). For 86 out of 377 inpatient deaths, the adverse event is so severe that it contributes to death. 27.9% of severe adverse events contributing to death originate in primary care. Lower respiratory infections (p<0.001, RR 2.81, 95% CI 1.76 to 4.51), medication harm (p<0.001, RR 5.21, 95% CI 3.04 to 8.94) and pressure ulcers (p=0.04, RR 2.23, 95% CI 1.03 to 4.85) are significantly more frequent for inpatient deaths than in the general sample of hospital patients.
Conclusions: Patients dying in hospitals experience seven times the rate of severe adverse events. Reviewing all inpatient death by the Global Trigger Tool method discloses new valid and reliable data of severe adverse events contributing to death which otherwise would be undetected.
Keywords: adverse events; global trigger tool; in-patient deaths; mortality.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical