

SGLT2 inhibition to address the unmet needs in diabetic nephropathy
- PMID: 30997935
- PMCID: PMC6849789
- DOI: 10.1002/dmrr.3171
SGLT2 inhibition to address the unmet needs in diabetic nephropathy
Abstract
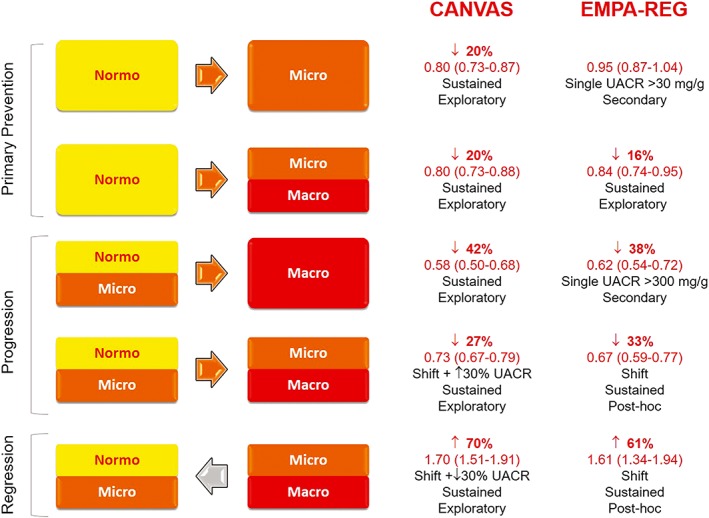
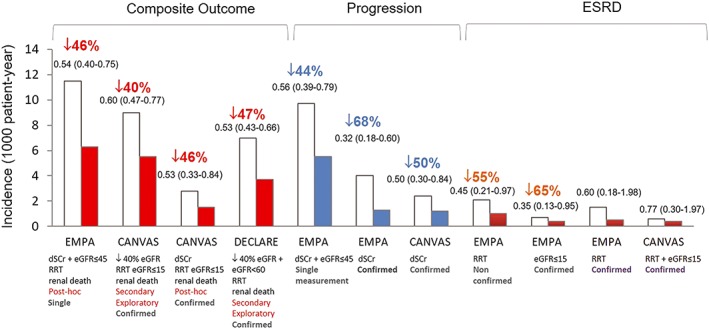
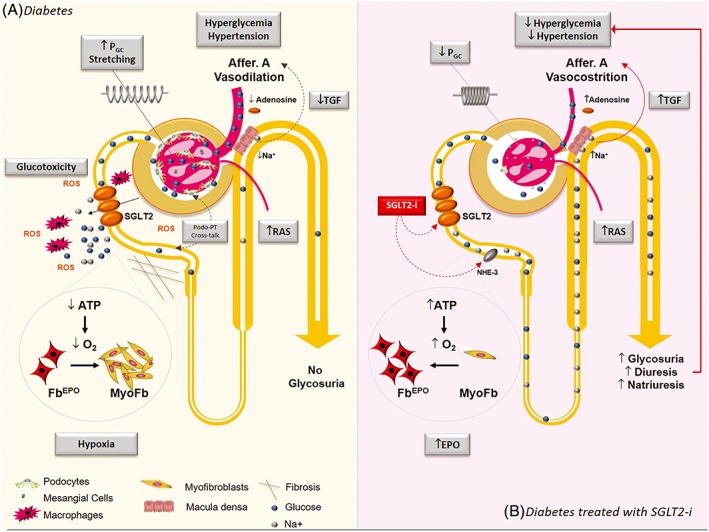
Current treatment of diabetic nephropathy is effective; however, substantial gaps in care still remain and new therapies are urgently needed to reduce the global burden of the complication. Desirable properties of an "ideal" new drug should include primary prevention of microalbuminuria, additive/synergistic anti-proteinuric effect in combination therapy with renin angiotensin system blockers, reduction of chronic kidney disease progression to lower the risk of end-stage renal disease, and cardiovascular protection. Growing evidence suggests that sodium-glucose cotransporter 2 inhibitors (SGLT2i) may fulfil many of these criteria and represent novel tools to cover the unmet needs in diabetic nephropathy care. However, the underlying mechanisms of SGLT2i renal benefits are still poorly understood and promising results from cardiovascular outcome trials with SGLT2i need confirmation in dedicated renal outcome trials.
Keywords: GFR; SGLT2; albuminuria; diabetic nephropathy; experimental diabetes.
© 2019 The Authors. Diabetes/Metabolism Research and Reviews Published by John Wiley & Sons Ltd.
Conflict of interest statement
Gruden G. has received a speaker fee from MundiPharma.
Figures
References
-
- Levin A, Tonelli M, Bonventre J, et al. Global kidney health 2017 and beyond: a roadmap for closing gaps in care, research, and policy. Lancet. 2017;390(10105):1888‐1917. - PubMed
-
- Brenner BM, Cooper ME, de Zeeuw D, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med. 2001;345(12):861‐869. - PubMed
-
- Lewis EJ, Hunsicker LG, Bain RP, Rohde RD. The effect of angiotensin‐converting‐enzyme inhibition on diabetic nephropathy. The collaborative study group. N Engl J Med. 1993;329(20):1456‐1462. - PubMed
