

The epidemiology of aerobic physical activity and muscle-strengthening activity guideline adherence among 383,928 U.S. adults
- PMID: 30999896
- PMCID: PMC6472085
- DOI: 10.1186/s12966-019-0797-2
The epidemiology of aerobic physical activity and muscle-strengthening activity guideline adherence among 383,928 U.S. adults
Abstract
Background: The World Health Organization's 'Global Recommendations on Physical Activity for Health' state that adults should engage in regular moderate-to-vigorous intensity aerobic physical activity (MVPA; e.g. walking, running, cycling) and muscle-strengthening activity (MSA; e.g. strength/resistance training). However, assessment of both MVPA and MSA is rare in physical activity surveillance. The aim of this study is to describe the prevalence, correlates and chronic health conditions associated with meeting the combined MVPA-MSA guidelines among a population representative sample of U.S. adults.
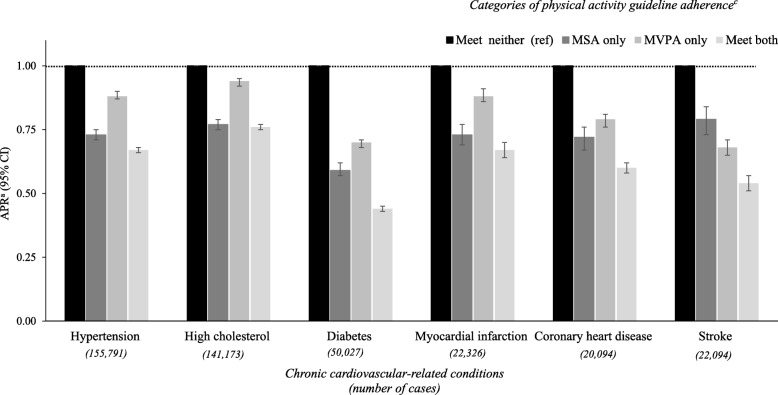
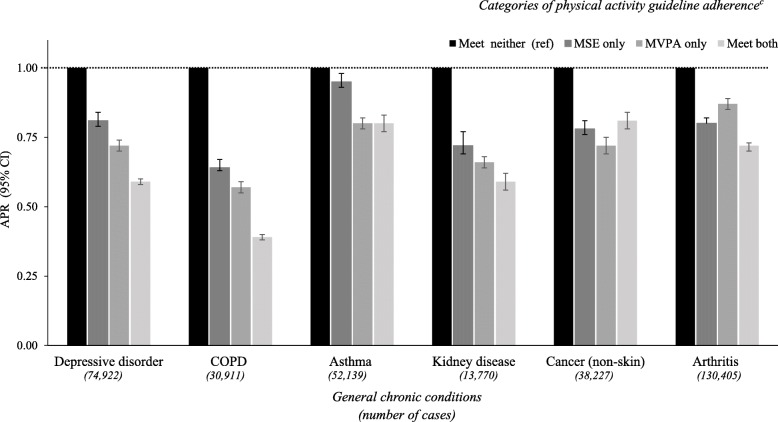
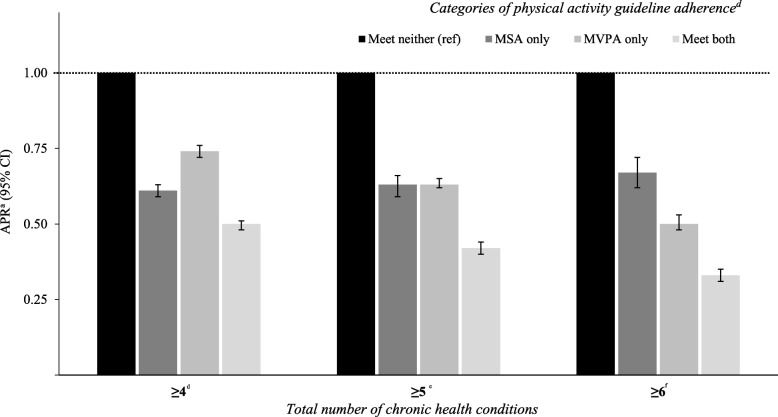
Methods: In this cross-sectional study, data were drawn from the U.S. 2015 Behavioral Risk Factor Surveillance System. During telephone interviews, MVPA and MSA were assessed using validated questionnaires. We calculated the proportions meeting both the global MVPA and MSA physical activity guidelines (MVPA ≥150 min/week and MSA ≥2 sessions/week). Poisson regressions with a robust error variance were used to assess: (i) prevalence ratios (PR) for meeting both guidelines across sociodemographic factors (e.g. age, sex, education, income, race/ethnicity); and (ii) PRs of 12 common chronic health conditions (e.g. diabetes, coronary heart disease, hypertension, depression) across different categories of physical activity guideline adherence (met neither [reference]; MSA only; MVPA only; met both).
Results: Among 383,928 adults (aged 18-80 years), 23.5% (95% CI: 20.1, 20.6%) met the combined MVPA-MSA guidelines. Those with poorer self-rated health, older adults, women, lower education/income and current smokers were less likely to meet the combined guidelines. After adjustment for covariates (e.g. age, self-rated health, income, smoking) compared with meeting neither guidelines, MSA only and MVPA only, meeting the combined MVPA-MSA guidelines was associated with the lowest PRs for all health conditions (APR range: 0.44-0.76), and the clustering of ≥6 chronic health conditions (APR = 0.33; 95% CI: 0.31-0.35).
Conclusions: Eight out of ten U.S. adults do not meet the global physical activity guidelines. This study supports the need for comprehensive health promotion strategies to increase the uptake and adherence of MVPA-MSA among U.S. adults. Large-scale interventions should target specific population sub-groups including older adults, women, those with poorer health and lower education/income.
Keywords: Aerobic exercise; Concurrent training; Physical activity; Public health; Resistance training.
Conflict of interest statement
Ethics approval and consent to participate
The Behavioral Risk Factor Surveillance System 2015 was approved by the National Center for Health Statistics Research Ethics Review Board and all the participants provided informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
