

Time for a reassessment of the treatment of hypothyroidism
- PMID: 30999905
- PMCID: PMC6471951
- DOI: 10.1186/s12902-019-0365-4
Time for a reassessment of the treatment of hypothyroidism
Abstract
Background: In the treatment for hypothyroidism, a historically symptom-orientated approach has given way to reliance on a single biochemical parameter, thyroid stimulating hormone (TSH).
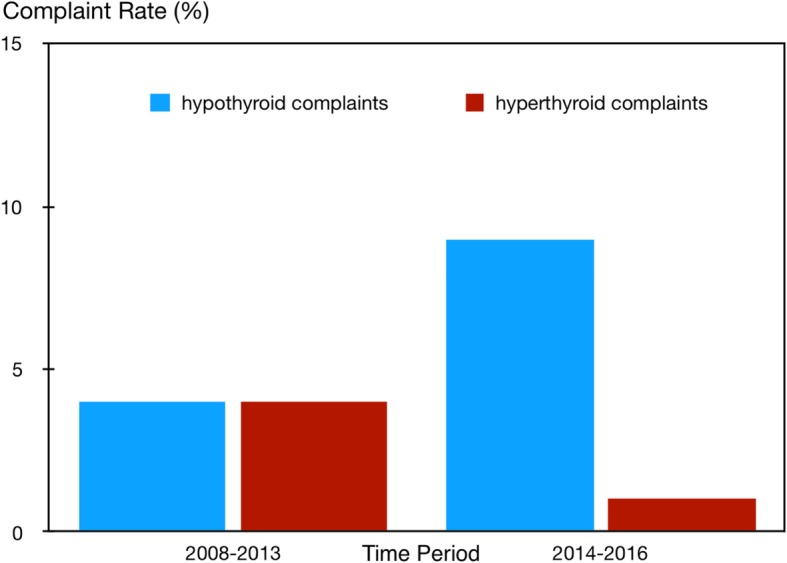
Main body: The historical developments and motivation leading to that decision and its potential implications are explored from pathophysiological, clinical and statistical viewpoints. An increasing frequency of hypothyroid-like complaints is noted in patients in the wake of this directional shift, together with relaxation of treatment targets. Recent prospective and retrospective studies suggested a changing pattern in patient complaints associated with recent guideline-led low-dose policies. A resulting dramatic rise has ensued in patients, expressing in various ways dissatisfaction with the standard treatment. Contributing factors may include raised problem awareness, overlap of thyroid-related complaints with numerous non-specific symptoms, and apparent deficiencies in the diagnostic process itself. Assuming that maintaining TSH anywhere within its broad reference limits may achieve a satisfactory outcome is challenged. The interrelationship between TSH, free thyroxine (FT4) and free triiodothyronine (FT3) is patient specific and highly individual. Population-based statistical analysis is therefore subject to amalgamation problems (Simpson's paradox, collider stratification bias). This invalidates group-averaged and range-bound approaches, rather demanding a subject-related statistical approach. Randomised clinical trial (RCT) outcomes may be equally distorted by intra-class clustering. Analytical distinction between an averaged versus typical outcome becomes clinically relevant, because doctors and patients are more interested in the latter. It follows that population-based diagnostic cut-offs for TSH may not be an appropriate treatment target. Studies relating TSH and thyroid hormone concentrations to adverse effects such as osteoporosis and atrial fibrillation invite similar caveats, as measuring TSH within the euthyroid range cannot substitute for FT4 and FT3 concentrations in the risk assessment. Direct markers of thyroid tissue effects and thyroid-specific quality of life instruments are required, but need methodological improvement.
Conclusion: It appears that we are witnessing a consequential historic shift in the treatment of thyroid disease, driven by over-reliance on a single laboratory parameter TSH. The focus on biochemistry rather than patient symptom relief should be re-assessed. A joint consideration together with a more personalized approach may be required to address the recent surge in patient complaint rates.
Keywords: Diagnostic strategies; Free thyroxine; Free triiodothyronine; Statistical analysis; Thyroid stimulating hormone; Thyroxine therapy; Treatment protocols, Randomised clinical trials.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
JWD received funding and personal fees by Sanofi-Henning, Bristol-Myers Squibb, Hexal AG and Pfizer, and is co-owner of the intellectual property rights for the patent “System and Method for Deriving Parameters for Homeostatic Feedback Control of an Individual” (Singapore Institute for Clinical Sciences, Biomedical Sciences Institutes, Application Number 201208940–5, WIPO number WO/2014/088516). All other authors declare that they have no competing interests and there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Study protocol; Thyroid hormone Replacement for Untreated older adults with Subclinical hypothyroidism - a randomised placebo controlled Trial (TRUST).BMC Endocr Disord. 2017 Feb 3;17(1):6. doi: 10.1186/s12902-017-0156-8. BMC Endocr Disord. 2017. PMID: 28158982 Free PMC article. Clinical Trial.
-
Free thyroxine, free triiodothyronine, and thyrotropin concentrations in hypothyroid and thyroid carcinoma patients receiving thyroxine therapy.Acta Endocrinol (Copenh). 1987 Nov;116(3):418-24. doi: 10.1530/acta.0.1160418. Acta Endocrinol (Copenh). 1987. PMID: 3687325
-
Symptomatic Relief is Related to Serum Free Triiodothyronine Concentrations during Follow-up in Levothyroxine-Treated Patients with Differentiated Thyroid Cancer.Exp Clin Endocrinol Diabetes. 2018 Sep;126(9):546-552. doi: 10.1055/s-0043-125064. Epub 2018 Feb 2. Exp Clin Endocrinol Diabetes. 2018. PMID: 29396968
-
ITALIAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS STATEMENT-REPLACEMENT THERAPY FOR PRIMARY HYPOTHYROIDISM: A BRIEF GUIDE FOR CLINICAL PRACTICE.Endocr Pract. 2016 Nov;22(11):1319-1326. doi: 10.4158/EP161308.OR. Epub 2016 Aug 2. Endocr Pract. 2016. PMID: 27482609 Review.
-
Hypothyroidism in the elderly: pathophysiology, diagnosis and treatment.Drugs Aging. 2005;22(1):23-38. doi: 10.2165/00002512-200522010-00002. Drugs Aging. 2005. PMID: 15663347 Review.
Cited by
-
Evidence-Based Use of Levothyroxine/Liothyronine Combinations in Treating Hypothyroidism: A Consensus Document.Eur Thyroid J. 2021 Mar;10(1):10-38. doi: 10.1159/000512970. Epub 2021 Feb 16. Eur Thyroid J. 2021. PMID: 33777817 Free PMC article.
-
Evaluating health outcomes in the treatment of hypothyroidism.Front Endocrinol (Lausanne). 2022 Oct 18;13:1026262. doi: 10.3389/fendo.2022.1026262. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36329885 Free PMC article. Review.
-
Clinical thyroidology: beyond the 1970s' TSH-T4 Paradigm.Front Endocrinol (Lausanne). 2025 Jun 24;16:1529791. doi: 10.3389/fendo.2025.1529791. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40630099 Free PMC article. Review.
-
Hypothyroidism - A Causal Approach to Testing Assumptions against Empirical Results.AMIA Jt Summits Transl Sci Proc. 2021 May 17;2021:257-266. eCollection 2021. AMIA Jt Summits Transl Sci Proc. 2021. PMID: 34457140 Free PMC article.
-
The Two Faces of Janus: Why Thyrotropin as a Cardiovascular Risk Factor May Be an Ambiguous Target.Front Endocrinol (Lausanne). 2020 Oct 26;11:542710. doi: 10.3389/fendo.2020.542710. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 33193077 Free PMC article.
References
-
- Gull WW. On a cretinoid state supervening in adult life in women. Trans Clin Soc London. 1874;7:180–185.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
