

Idiopathic intracranial hypertension presenting with isolated unilateral facial nerve palsy: a case report
- PMID: 30999940
- PMCID: PMC6474063
- DOI: 10.1186/s13256-019-2060-5
Idiopathic intracranial hypertension presenting with isolated unilateral facial nerve palsy: a case report
Abstract
Background: Idiopathic intracranial hypertension, also known as pseudotumor cerebri, is a disorder characterized by increased intracranial pressure of unclear pathogenesis in the absence of other structural and obstructive lesions that is predominantly, although not exclusively, seen in obese women of childbearing age. Patients with idiopathic intracranial hypertension commonly present with a headache, transient visual obscurations, and intracranial noises with some cranial nerves occasionally involved, most commonly CN VI. We report idiopathic intracranial hypertension presenting with isolated complete unilateral facial nerve palsy, as the sole cranial nerve involved, which is a presentation rarely reported in the literature.
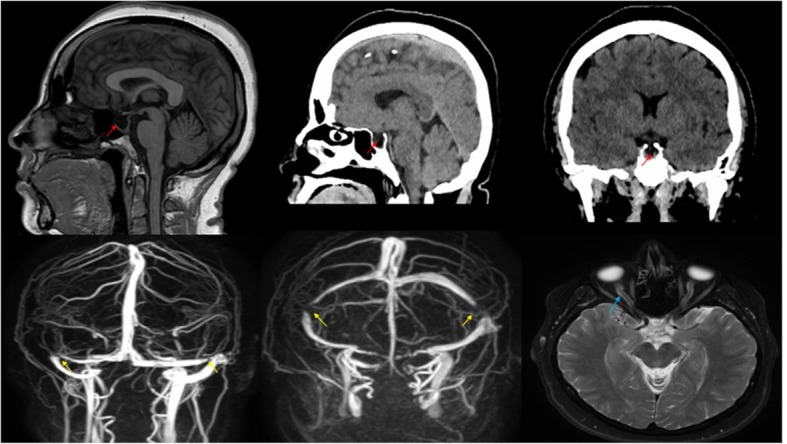
Case presentation: A 40-year-old Hispanic woman with a history of obesity and hypertension presented to our emergency department complaining of bifrontal headache for 3 days associated with nausea, vomiting, transient visual disturbances, and a picture of right-sided cranial nerve VII palsy. Her neurologic examination including other cranial nerves was otherwise normal, but a fundus examination revealed bilateral grade II papilledema. Imaging studies ruled out structural and obstructive lesions as possible causes of her symptoms and lumber puncture results were unremarkable except for an increased opening pressure. She was then started on prednisone and acetazolamide. Two days later, she reported a dramatic improvement in both headache and facial nerve palsy.
Conclusions: Idiopathic intracranial hypertension should be suspected in obese young women presenting with headache and transient visual complaints and some cranial nerve abnormalities. Idiopathic intracranial hypertension is a diagnosis of exclusion and imaging studies should always be performed to rule out other structural and obstructive lesions. In this case report, we aimed to draw attention to the possibility of idiopathic intracranial hypertension presenting with unilateral cranial nerve VII palsy as the only cranial nerve involved, which needs a high index of suspicion by clinicians. The mechanisms of cranial nerve VII palsy in idiopathic intracranial hypertension are not well understood and prompt further investigation.
Keywords: Anatomical correlation; CN VII palsy; IIH; Rare association.
Conflict of interest statement
Ethics approval and consent to participate
Ethics committee approval was not applicable as the information was analyzed in a retrospective manner and had no effect on treatment.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
