

Treatment of malignant pleural effusions: the case for localized immunotherapy
- PMID: 30999958
- PMCID: PMC6472034
- DOI: 10.1186/s40425-019-0590-4
Treatment of malignant pleural effusions: the case for localized immunotherapy
Abstract
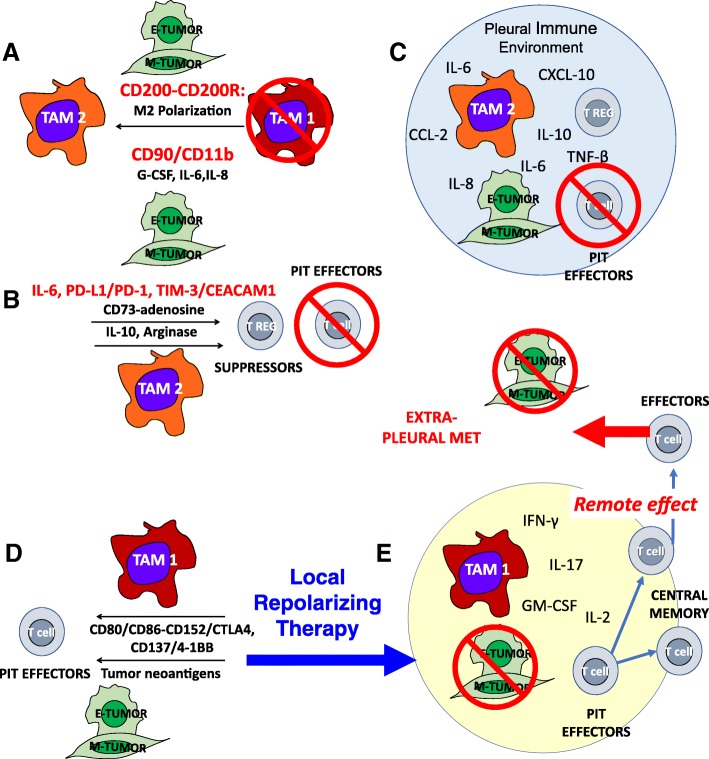
Malignant pleural effusions (MPE) are a common terminal pathway for many cancers, with an estimated United States incidence of more than 150,000 cases per year. MPE is an aggressive disease with a uniformly fatal prognosis and a life expectancy of only 3 to 12 months. The development of an effective targeted therapy represents a pressing unmet need. This commentary focuses on how cellular and humoral components condition the pleural space as a tumor-promoting, wound-healing environment. Despite an abundance of potential antigen presenting and effector cells in the pleura, their physical isolation by the mesothelial barrier, the concentration of cytokines and chemokines driving the epithelial to mesenchymal transition (EMT) and M2 /Th-2 polarization, suppress tumor-specific immune effector responses. We argue that local immune repolarization must precede either immune checkpoint or cellular therapy to successfully eradicate pleural tumor. We further hypothesize that, because of its cellular content, a repolarized pleural space will provide an effective immune environment for generation of systemic anti-tumor response.
Keywords: Immunotherapy; Malignant pleural effusion; Pleural infiltrating T cells (PIT); Tumor associated macrophages (TAM).
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
All authors consent.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources