

Percutaneous Coronary Intervention in Older Patients With ST-Segment Elevation Myocardial Infarction and Cardiogenic Shock
- PMID: 30999991
- PMCID: PMC7185801
- DOI: 10.1016/j.jacc.2019.01.055
Percutaneous Coronary Intervention in Older Patients With ST-Segment Elevation Myocardial Infarction and Cardiogenic Shock
Abstract
Background: Older adults ≥75 years of age carry an increased risk of mortality after ST-segment elevation myocardial infarction (STEMI) complicated by cardiogenic shock.
Objectives: The purpose of this study was to examine the use of percutaneous coronary intervention (PCI) in older adults with STEMI and shock and its influence on in-hospital mortality.
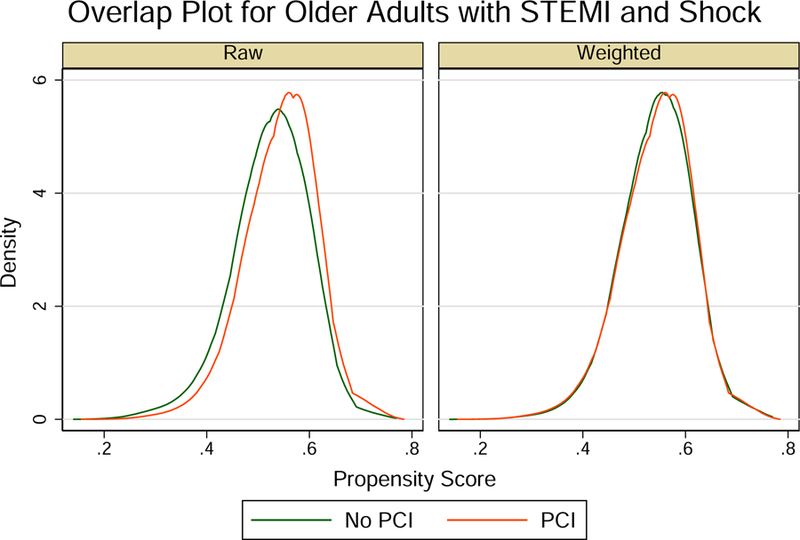
Methods: We used a large publicly available all-payer inpatient health care database sponsored by the Agency for Healthcare Research and Quality between 1999 and 2013. The primary outcome was in-hospital mortality. The influence of PCI on in-hospital mortality was assessed by quintiles of propensity score (PS).
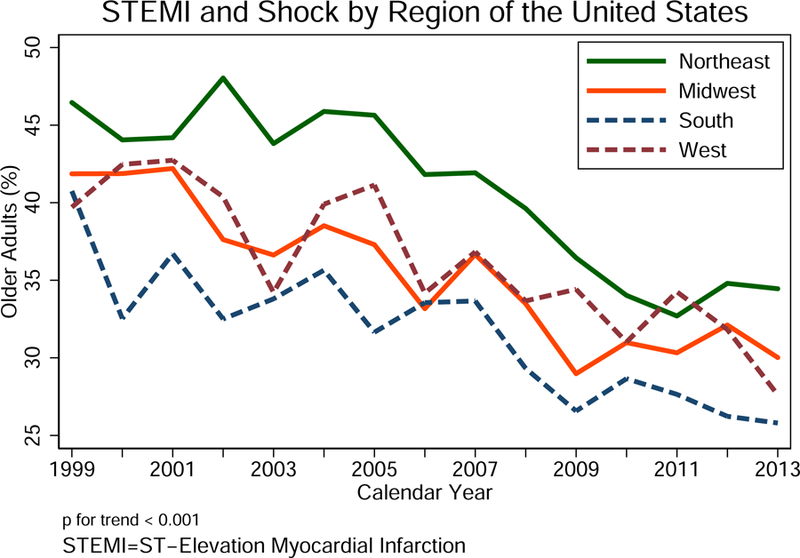
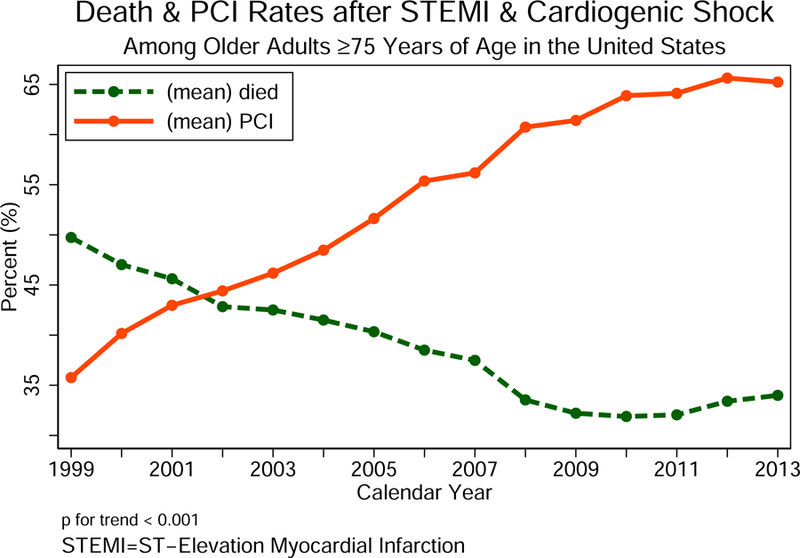
Results: Of the 317,728 encounters with STEMI and shock in the United States, 111,901 (35%) were adults age ≥75 years. Of these, 53% were women and 83% were Caucasians. The median number of chronic conditions was 8 (interquartile range: 6 to 10). The diagnosis of STEMI and cardiogenic shock in older patients decreased significantly over time (proportion of older adults with STEMI and shock: 1999: 42% vs. 2013: 29%). Concomitantly, the rate of PCI utilization in older adults increased (1999: 27% vs. 2013: 56%, p < 0.001), with declining in-hospital mortality rates (1999: 64% vs. 2013: 46%; p < 0.001). Utilizing PS matching methods, PCI was associated with a lower risk of in-hospital mortality across quintiles of propensity score (Mantel-Haenszel odds ratio: 0.48; 95% confidence interval [CI]: 0.45 to 0.51). This reduction in hospital mortality risk was seen across the 4 different U.S. census bureau regions (adjusted odds ratio: Northeast: 0.41; 95% CI: 0.36 to 0.47; Midwest: 0.49; 95% CI: 0.42 to 0.57; South: 0.51; 95% CI: 0.46 to 0.56; West: 0.46; 95% CI: 0.41 to 0.53).
Conclusions: This large and contemporary analysis shows that utilization of PCI in older adults with STEMI and cardiogenic shock is increasing and paralleled by a substantial reduction in mortality. Although clinical judgment is critical, older adults should not be excluded from early revascularization based on age in the absence of absolute contraindications.
Keywords: ST-segment elevation myocardial infarction; cardiogenic shock; mortality; older adults; percutaneous coronary intervention.
Copyright © 2019 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures


Comment in
-
Age, STEMI, and Cardiogenic Shock: Never Too Old for PCI?J Am Coll Cardiol. 2019 Apr 23;73(15):1901-1904. doi: 10.1016/j.jacc.2018.12.088. J Am Coll Cardiol. 2019. PMID: 30999992 No abstract available.
References
-
- Mozaffarian D, Benjamin EJ, Go AS et al. Executive Summary: Heart Disease and Stroke Statistics−-2016 Update: A Report From the American Heart Association. Circulation 2016;133:447–54. - PubMed
-
- Damluji AA, Ramireddy A, Forman DE. Management and Care of Older Cardiac Patients. In: Vasan RS, Sawyer DB, editors. Encyclopedia of Cardiovascular Research and Medicine Oxford: Elsevier, 2018:245–265.
-
- Alexander KP, Newby LK, Armstrong PW et al. Acute coronary care in the elderly, part II: ST-segment-elevation myocardial infarction: a scientific statement for healthcare professionals from the American Heart Association Council on Clinical Cardiology: in collaboration with the Society of Geriatric Cardiology. Circulation 2007;115:2570–89. - PubMed
-
- Thompson CR, Buller CE, Sleeper LA et al. Cardiogenic shock due to acute severe mitral regurgitation complicating acute myocardial infarction: a report from the SHOCK Trial Registry. SHould we use emergently revascularize Occluded Coronaries in cardiogenic shocK? J Am Coll Cardiol 2000;36:1104–9. - PubMed
-
- Menon V, Webb JG, Hillis LD et al. Outcome and profile of ventricular septal rupture with cardiogenic shock after myocardial infarction: a report from the SHOCK Trial Registry. SHould we emergently revascularize Occluded Coronaries in cardiogenic shocK? J Am Coll Cardiol 2000;36:1110–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
