

Predicting Motor Outcome in Acute Intracerebral Hemorrhage
- PMID: 31000524
- PMCID: PMC7053898
- DOI: 10.3174/ajnr.A6038
Predicting Motor Outcome in Acute Intracerebral Hemorrhage
Abstract
Background and purpose: Predicting motor outcome following intracerebral hemorrhage is challenging. We tested whether the combination of clinical scores and DTI-based assessment of corticospinal tract damage within the first 12 hours of symptom onset after intracerebral hemorrhage predicts motor outcome at 3 months.
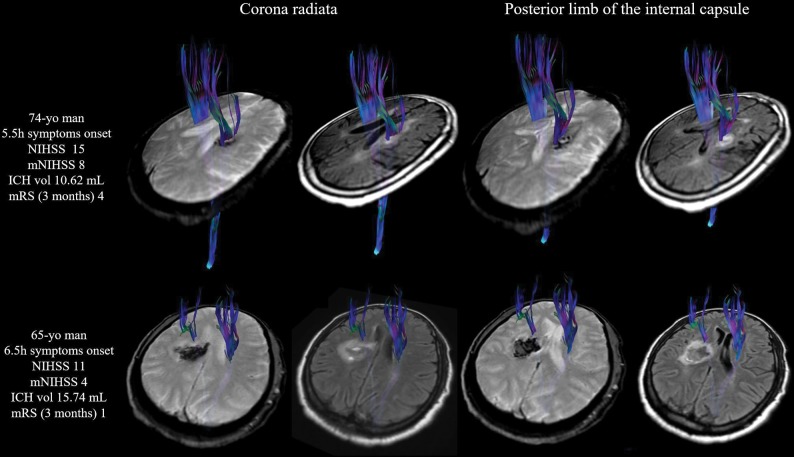
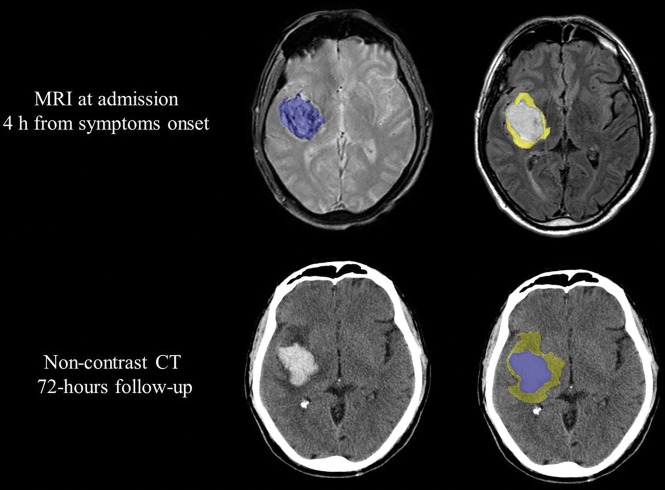
Materials and methods: We prospectively studied patients with motor deficits secondary to primary intracerebral hemorrhage within the first 12 hours of symptom onset. Patients underwent multimodal MR imaging including DTI. We assessed intracerebral hemorrhage and perihematomal edema location and volume, and corticospinal tract involvement. The corticospinal tract was considered affected when the tractogram passed through the intracerebral hemorrhage or/and the perihematomal edema. We also calculated affected corticospinal tract-to-unaffected corticospinal tract ratios for fractional anisotropy, mean diffusivity, and axial and radial diffusivities. Motor impairment was graded by the motor subindex scores of the modified NIHSS. Motor outcome at 3 months was classified as good (modified NIHSS 0-3) or poor (modified NIHSS 4-8).
Results: Of 62 patients, 43 were included. At admission, the median NIHSS score was 13 (interquartile range = 8-17), and the median modified NIHSS score was 5 (interquartile range = 2-8). At 3 months, 13 (30.23%) had poor motor outcome. Significant independent predictors of motor outcome were NIHSS and modified NIHSS at admission, posterior limb of the internal capsule involvement by intracerebral hemorrhage at admission, intracerebral hemorrhage volume at admission, 72-hour NIHSS, and 72-hour modified NIHSS. The sensitivity, specificity, and positive and negative predictive values for poor motor outcome at 3 months by a combined modified NIHSS of >6 and posterior limb of the internal capsule involvement in the first 12 hours from symptom onset were 84%, 79%, 65%, and 92%, respectively (area under the curve = 0.89; 95% CI, 0.78-1).
Conclusions: Combined assessment of motor function and posterior limb of the internal capsule damage during acute intracerebral hemorrhage accurately predicts motor outcome.
© 2019 by American Journal of Neuroradiology.
Figures
Similar articles
-
Natural history and prognostic value of corticospinal tract Wallerian degeneration in intracerebral hemorrhage.J Am Heart Assoc. 2013 Aug 2;2(4):e000090. doi: 10.1161/JAHA.113.000090. J Am Heart Assoc. 2013. PMID: 23913508 Free PMC article.
-
Diffusion tensor tractography predicts motor functional outcome in patients with spontaneous intracerebral hemorrhage.Neurosurgery. 2008 Jan;62(1):97-103; discussion 103. doi: 10.1227/01.NEU.0000311066.03121.B8. Neurosurgery. 2008. PMID: 18300896
-
Motor outcome of deep intracerebral haemorrhage in diffusion tensor imaging: comparison of data from different locations along the corticospinal tract.Neurol Res. 2015 Sep;37(9):774-81. doi: 10.1179/1743132815Y.0000000050. Epub 2015 May 25. Neurol Res. 2015. PMID: 26003992
-
Peri-hematoma corticospinal tract integrity in intracerebral hemorrhage patients: A diffusion-tensor imaging study.J Neurol Sci. 2021 Feb 15;421:117317. doi: 10.1016/j.jns.2021.117317. Epub 2021 Jan 12. J Neurol Sci. 2021. PMID: 33476986
-
Mechanism of White Matter Injury and Promising Therapeutic Strategies of MSCs After Intracerebral Hemorrhage.Front Aging Neurosci. 2021 Apr 13;13:632054. doi: 10.3389/fnagi.2021.632054. eCollection 2021. Front Aging Neurosci. 2021. PMID: 33927608 Free PMC article. Review.
Cited by
-
Cerebral arterial blood flow, attention, and executive and cognitive functions in depressed patients after acute hypertensive cerebral hemorrhage.World J Clin Cases. 2024 Jul 6;12(19):3815-3823. doi: 10.12998/wjcc.v12.i19.3815. World J Clin Cases. 2024. PMID: 38994304 Free PMC article.
-
Association between superior longitudinal fasciculus, motor recovery, and motor outcome after stroke: a cohort study.Front Neurol. 2023 Jul 14;14:1157625. doi: 10.3389/fneur.2023.1157625. eCollection 2023. Front Neurol. 2023. PMID: 37521287 Free PMC article.
-
Machine learning models predict coagulopathy in spontaneous intracerebral hemorrhage patients in ER.CNS Neurosci Ther. 2021 Jan;27(1):92-100. doi: 10.1111/cns.13509. Epub 2020 Nov 28. CNS Neurosci Ther. 2021. PMID: 33249760 Free PMC article.
-
Remodeling and Characterization Analysis of Corticospinal Tract in Patients with Intracerebral Hemorrhage in the Basal Ganglia.Transl Stroke Res. 2025 Oct;16(5):1550-1563. doi: 10.1007/s12975-025-01326-4. Epub 2025 Jan 9. Transl Stroke Res. 2025. PMID: 39786647
-
Acute corticospinal tract diffusion tensor imaging predicts 6-month functional outcome after intracerebral haemorrhage.J Neurol. 2022 Nov;269(11):6058-6066. doi: 10.1007/s00415-022-11245-1. Epub 2022 Jul 21. J Neurol. 2022. PMID: 35861854 Free PMC article.