

A functional Magnetic Resonance Imaging study of patients with Polar Type II/III complex shoulder instability
- PMID: 31000752
- PMCID: PMC6472426
- DOI: 10.1038/s41598-019-42754-1
A functional Magnetic Resonance Imaging study of patients with Polar Type II/III complex shoulder instability
Abstract
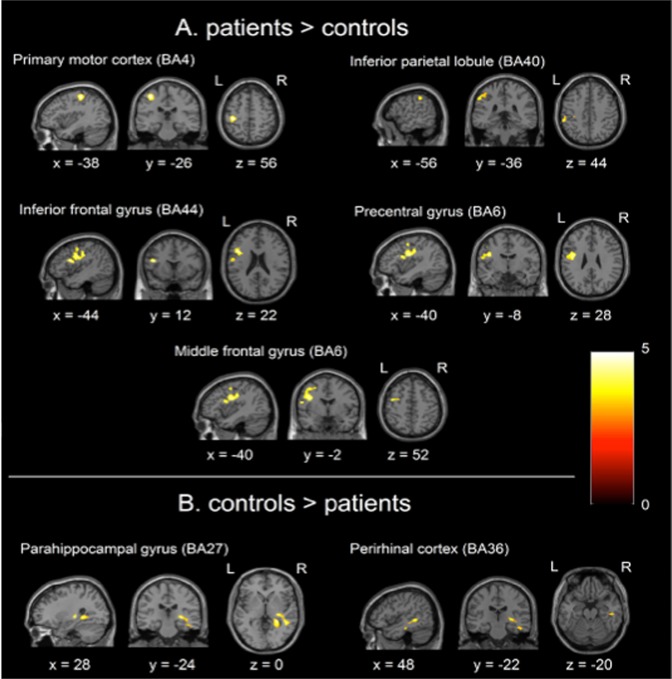
The pathophysiology of Stanmore Classification Polar type II/III shoulder instability is not well understood. Functional Magnetic Resonance Imaging was used to measure brain activity in response to forward flexion and abduction in 16 patients with Polar Type II/III shoulder instability and 16 age-matched controls. When a cluster level correction was applied patients showed significantly greater brain activity than controls in primary motor cortex (BA4), supramarginal gyrus (BA40), inferior frontal gyrus (BA44), precentral gyrus (BA6) and middle frontal gyrus (BA6): the latter region is considered premotor cortex. Using voxel level correction within these five regions a unique activation was found in the primary motor cortex (BA4) at MNI coordinates -38 -26 56. Activation was greater in controls compared to patients in the parahippocampal gyrus (BA27) and perirhinal cortex (BA36). These findings show, for the first time, neural differences in patients with complex shoulder instability, and suggest that patients are in some sense working harder or differently to maintain shoulder stability, with brain activity similar to early stage motor sequence learning. It will help to understand the condition, design better therapies and improve treatment of this group; avoiding the common clinical misconception that their recurrent shoulder dislocations are a form of attention-seeking.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Neural Correlates of Clinical Scores in Patients with Anterior Shoulder Apprehension.Med Sci Sports Exerc. 2015 Dec;47(12):2612-20. doi: 10.1249/MSS.0000000000000726. Med Sci Sports Exerc. 2015. PMID: 26110696
-
Altered grey matter volume and cortical thickness in patients with schizo-obsessive comorbidity.Psychiatry Res Neuroimaging. 2018 Jun 30;276:65-72. doi: 10.1016/j.pscychresns.2018.03.009. Epub 2018 Mar 28. Psychiatry Res Neuroimaging. 2018. PMID: 29628272
-
Structural and cognitive correlates of fatigue in progressive multiple sclerosis.Neurol Res. 2019 Feb;41(2):168-176. doi: 10.1080/01616412.2018.1547813. Epub 2018 Dec 4. Neurol Res. 2019. PMID: 30513278
-
Disentangling Mathematics from Executive Functions by Investigating Unique Functional Connectivity Patterns Predictive of Mathematics Ability.J Cogn Neurosci. 2019 Apr;31(4):560-573. doi: 10.1162/jocn_a_01367. Epub 2018 Dec 19. J Cogn Neurosci. 2019. PMID: 30566368
-
Magnetic Resonance Imaging and Arthroscopic Correlation in Shoulder Instability.Sports Med Arthrosc Rev. 2017 Dec;25(4):172-178. doi: 10.1097/JSA.0000000000000163. Sports Med Arthrosc Rev. 2017. PMID: 29095395 Review.
Cited by
-
Neuromuscular Electrical Stimulation-Enhanced Physical Therapist Intervention for Functional Posterior Shoulder Instability (Type B1): A Multicenter Randomized Controlled Trial.Phys Ther. 2024 Jan 1;104(1):pzad145. doi: 10.1093/ptj/pzad145. Phys Ther. 2024. PMID: 37870503 Free PMC article. Clinical Trial.
-
Functional cortical changes associated with shoulder instability - a systematic review.Shoulder Elbow. 2022 Aug;14(4):452-464. doi: 10.1177/17585732211019016. Epub 2021 Jun 10. Shoulder Elbow. 2022. PMID: 35846404 Free PMC article.
-
Shoulder-Pacemaker Treatment Concept for Posterior Positional Functional Shoulder Instability: A Prospective Clinical Trial.Am J Sports Med. 2020 Jul;48(9):2097-2104. doi: 10.1177/0363546520933841. Am J Sports Med. 2020. PMID: 32667266 Free PMC article. Clinical Trial.
-
Advances in the Non-Operative Management of Multidirectional Instability of the Glenohumeral Joint.J Clin Med. 2022 Aug 31;11(17):5140. doi: 10.3390/jcm11175140. J Clin Med. 2022. PMID: 36079068 Free PMC article.
-
Grading system for Hill-Sachs lesion and its association with Bankart lesion: a cross-sectional study.BMC Musculoskelet Disord. 2025 Jul 4;26(1):623. doi: 10.1186/s12891-025-08751-4. BMC Musculoskelet Disord. 2025. PMID: 40615958 Free PMC article.
References
-
- Lewis A, Kitamura T, Bayley J. The Classification of Shoulder Instability:new light through old windows. Current Orthopaedics. 2004;18:97–108. doi: 10.1016/j.cuor.2004.04.002. - DOI
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
