

Corrosive injuries of the upper gastrointestinal tract: A pictorial review of the imaging features
- PMID: 31000935
- PMCID: PMC6467036
- DOI: 10.4103/ijri.IJRI_349_18
Corrosive injuries of the upper gastrointestinal tract: A pictorial review of the imaging features
Abstract
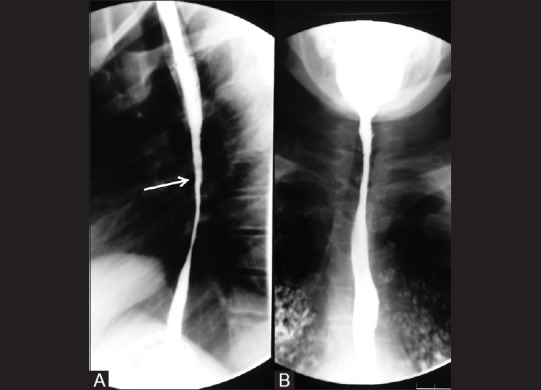
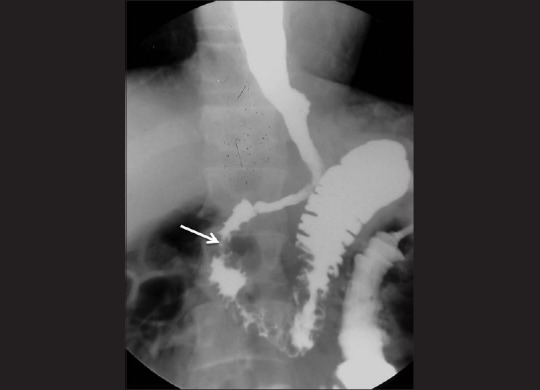
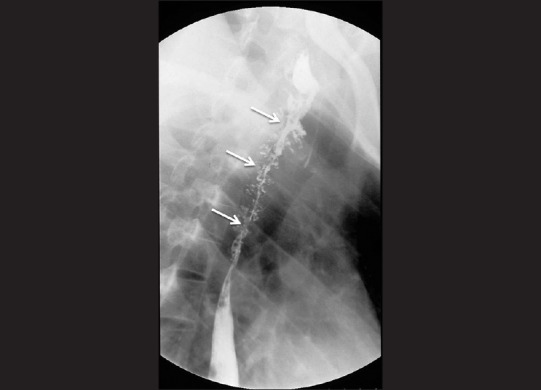
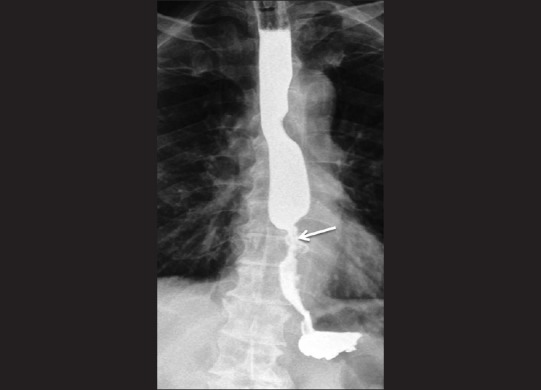
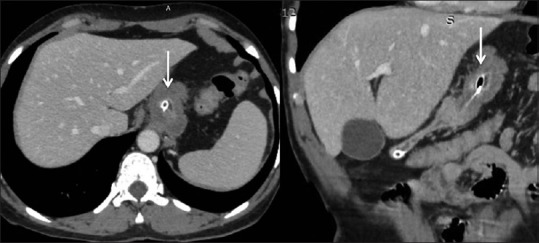
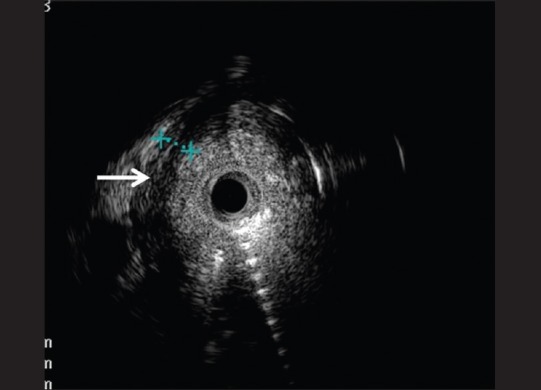
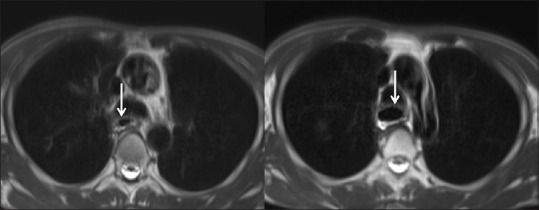
Corrosive ingestion is a common form of poisoning. Corrosive agents cause severe damage to the gastrointestinal (GI) tract. The most severe forms of injury can lead to mortality; however, the major concern with this type of injury is life-long morbidity. Upper GI endoscopy is the test of choice for assessing severity in the acute phase of the disease. The long-term management is based on the site, length, number, location, and tightness of the stricture. This information is best provided by the barium contrast studies. In this pictorial review, a spectrum of findings in patients with corrosive injuries of the esophagus and stomach is illustrated. The role of various imaging modalities including barium studies, endoscopic ultrasound, computed tomography, and magnetic resonance imaging is discussed.
Keywords: Barium; corrosive; stricture.
Conflict of interest statement
There are no conflicts of interest.
Figures











Similar articles
-
Radiological spectrum of late sequelae of corrosive injury to upper gastrointestinal tract. A pictorial review.Acta Radiol. 2004 Feb;45(1):7-12. doi: 10.1080/02841850410003329. Acta Radiol. 2004. PMID: 15164772
-
Post-corrosive injuries of upper gastrointestinal tract.Prilozi. 2010;31(1):297-316. Prilozi. 2010. PMID: 20693948
-
The clinical toxicology of sodium hypochlorite.Clin Toxicol (Phila). 2019 May;57(5):303-311. doi: 10.1080/15563650.2018.1543889. Epub 2019 Jan 28. Clin Toxicol (Phila). 2019. PMID: 30689457 Review.
-
Prediction of bleeding and stricture formation after corrosive ingestion by EUS concurrent with upper endoscopy.Gastrointest Endosc. 2004 Nov;60(5):827-33. doi: 10.1016/s0016-5107(04)02031-0. Gastrointest Endosc. 2004. PMID: 15557970
-
Corrosive injury to the upper gastrointestinal tract.Indian J Gastroenterol. 1993 Oct;12(4):135-41. Indian J Gastroenterol. 1993. PMID: 8270293 Review.
Cited by
-
Non gastro-esophageal reflux disease related esophagitis: an overview with a histologic diagnostic approach.Pathologica. 2020 Sep;112(3):128-137. doi: 10.32074/1591-951X-156. Pathologica. 2020. PMID: 33179617 Free PMC article. Review.
-
A Dreaded Complication of Corrosive Poisoning Leading to Gangrene of the Stomach and Duodenum: A Rare Case.Cureus. 2024 May 14;16(5):e60313. doi: 10.7759/cureus.60313. eCollection 2024 May. Cureus. 2024. PMID: 38882952 Free PMC article.
-
Of forgotten physicians, procedures, and principles.Indian J Thorac Cardiovasc Surg. 2023 Jul;39(4):428-430. doi: 10.1007/s12055-023-01496-6. Epub 2023 Mar 18. Indian J Thorac Cardiovasc Surg. 2023. PMID: 37346446 Free PMC article. No abstract available.
-
Corrosive injury of the upper gastrointestinal tract: the evolving role of a radiologist.Br J Radiol. 2020 Oct 1;93(1114):20200528. doi: 10.1259/bjr.20200528. Epub 2020 Jul 24. Br J Radiol. 2020. PMID: 32706982 Free PMC article. Review.
-
A caustic ingestion consequence mistaken for gastric cancer: A case report.Int J Surg Case Rep. 2020;75:100-103. doi: 10.1016/j.ijscr.2020.09.019. Epub 2020 Sep 8. Int J Surg Case Rep. 2020. PMID: 32932036 Free PMC article.
References
-
- Gumaste VV, Dave PB. Ingestion of corrosive substances by adults. Am J Gastroenterol. 1992;87:1–5. - PubMed
-
- Lakshmi CP, Vijayahari R, Kate V, Ananthakrishnan N. A hospital-based epidemiological study of corrosive alimentary injuries with particular reference to the Indian experience. Natl Med J India. 2013;26:31–6. - PubMed