

Subcutaneous emphysema, pneumothorax and pneumomediastinum as a complication of an asthma attack
- PMID: 31000946
- PMCID: PMC6467038
- DOI: 10.4103/ijri.IJRI_340_18
Subcutaneous emphysema, pneumothorax and pneumomediastinum as a complication of an asthma attack
Abstract
Introduction: Simultaneous subcutaneous emphysema, spontaneous pneumothorax, and pneumomediastinum are complications rarely observed synchronously during an acute exacerbation of bronchial asthma. Although spontaneous pneumothorax has already been reported in asthma patients in the literature, its concurrence with subcutaneous emphysema and pneumomediastinum is extremely rare except for iatrogenic conditions.
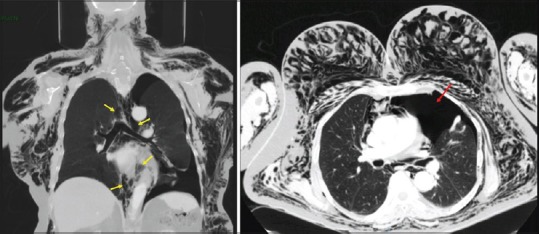
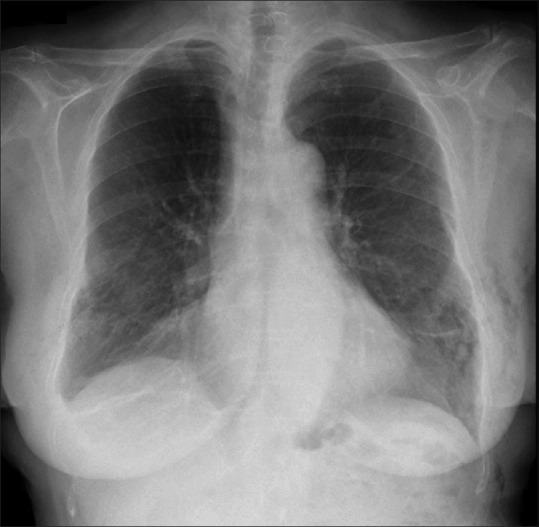
Case study: We describe a patient who presented to the emergency room with progressive dyspnea and chest pain. Three days before, she consulted her general physician with a history of violent dry cough and wheezing. An acute asthma exacerbation was diagnosed, and an inhaled short-acting beta 2 agonist and oral prednisone were prescribed. The patient developed simultaneous subcutaneous emphysema, spontaneous pneumothorax, and pneumomediastinum, a rare complication of an asthma attack.
Conclusions: Our aim is to emphasize that occult pneumothoraces should be considered in a patient presenting with an acute asthma attack failing to respond to conventional medical therapy.
Keywords: Asthma; pneumomediastinum; spontaneous pneumothorax; subcutaneous emphysema.
Conflict of interest statement
There are no conflicts of interest.
Figures

References
-
- Banki F, Estrera AL, Harrison RG, Miller CC, 3rd, Leake SS, Mitchell KG, et al. Pneumomediastinum: etiology and a guide to diagnosis and treatment. Am J Surg. 2013;206(6):1001–1006. - PubMed
-
- Maunder RJ, Pierson DJ, Hudson LD. Subcutaneous and mediastinal emphysema: pathophysiology, diagnosis, and management. Arch Intern Med. 1984;144(7):1447–1453. - PubMed