

Functional and Objective Audiovestibular Evaluation of Children With Apparent Semicircular Canal Dehiscence-A Case Series in a Pediatric Vestibular Center
- PMID: 31001191
- PMCID: PMC6454049
- DOI: 10.3389/fneur.2019.00306
Functional and Objective Audiovestibular Evaluation of Children With Apparent Semicircular Canal Dehiscence-A Case Series in a Pediatric Vestibular Center
Abstract
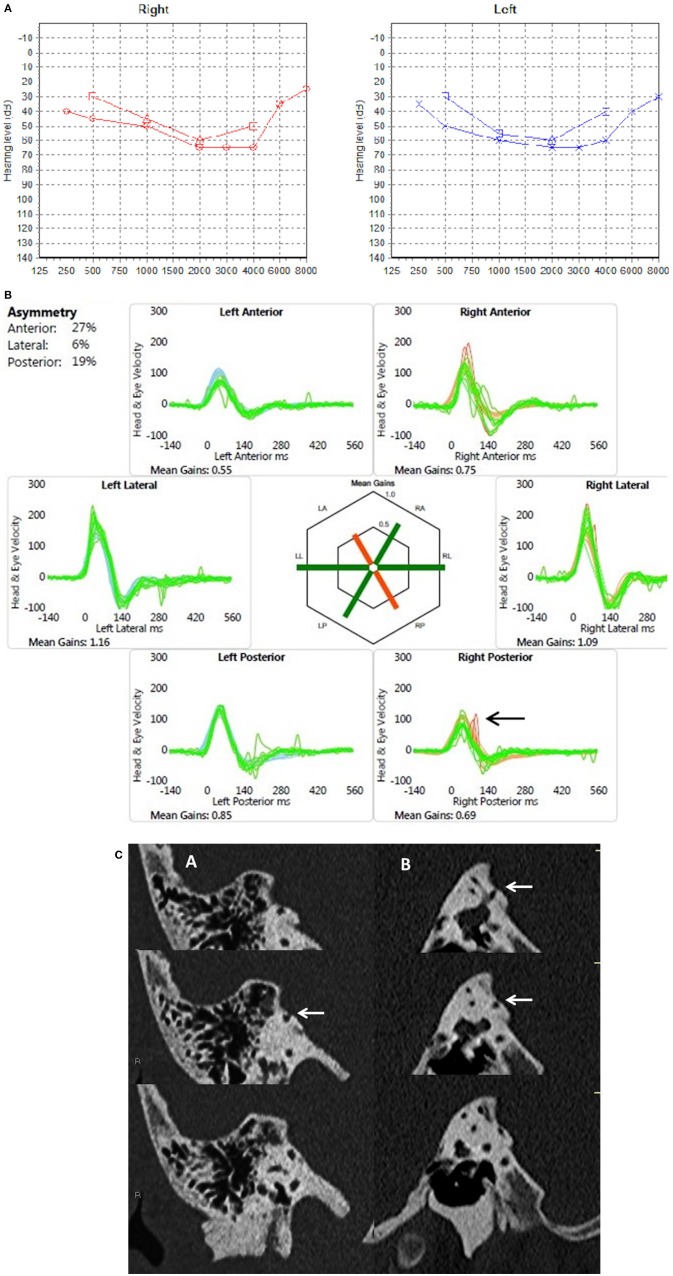
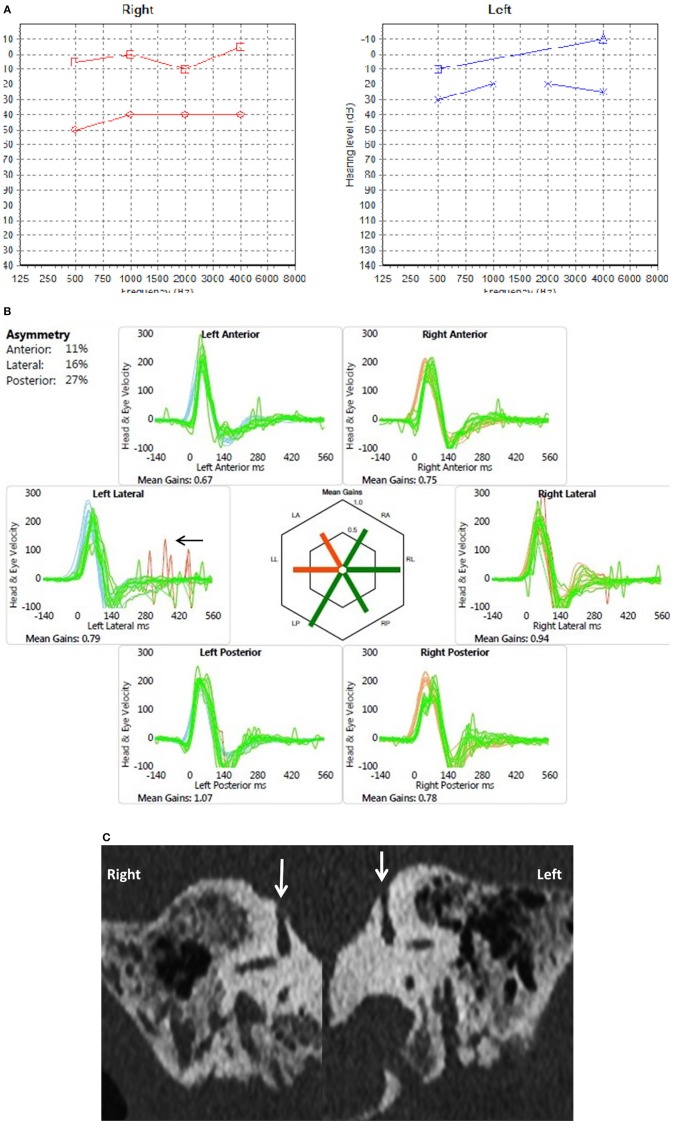
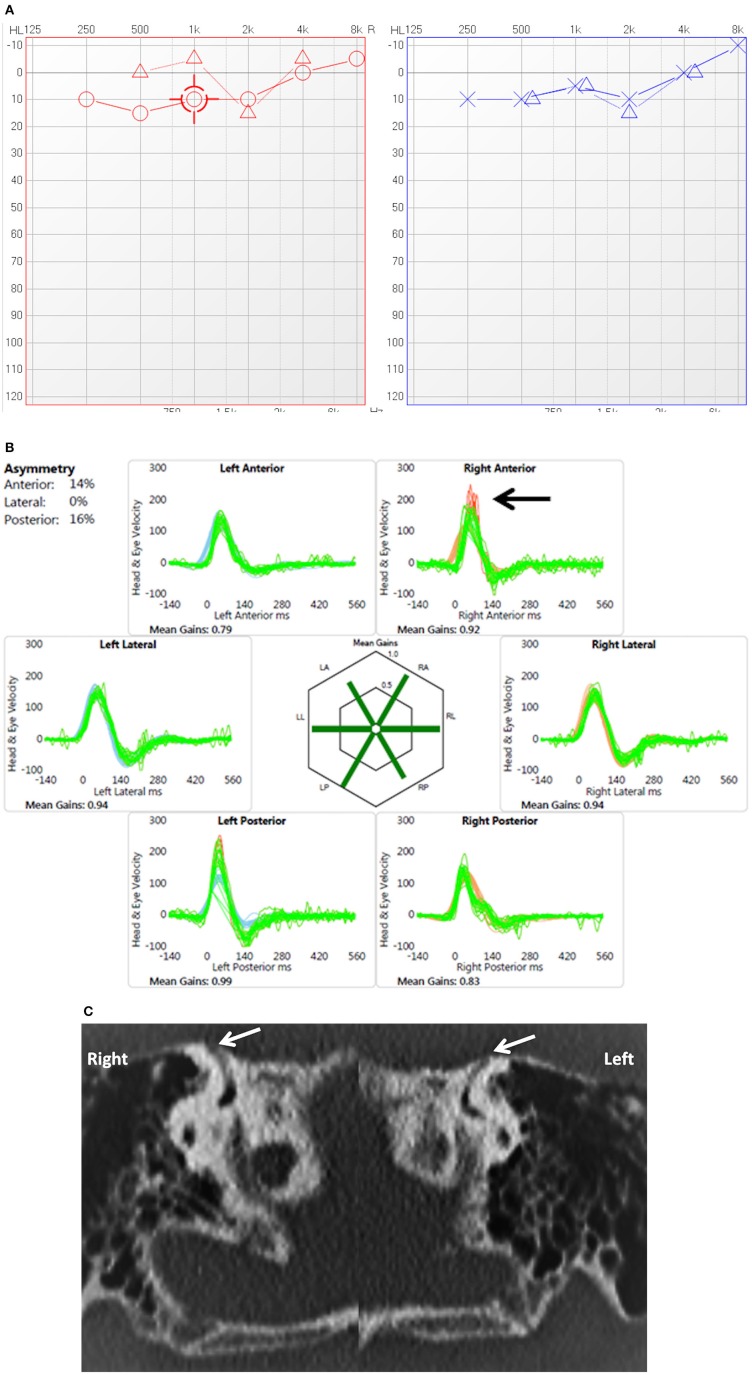
Semicircular canal dehiscence is a bony abnormality in the otic capsule especially involving the superior semicircular canal. Since its identification in 1998, there is significant research regarding the pathology in the adult population. This condition generates a third window effect that is well-described in the literature. However, the entity is rare in the pediatric population with limited research. Difficulties encountered in children are obtaining a direct history that is essential for the diagnosis followed by neurovestibular tests that may be difficult to perform. This study presents observations regarding different clinical and diagnostic aspects of semicircular canal dehiscences in children as a retrospective audit in a tertiary pediatric vestibular center. Of 580 children assessed in a 30 months period undergoing comprehensive functional and objective audiovestibular assessment, 13 children (2.2%) were detected to possess radiological semicircular canal dehiscences (high resolution computed tomography scans at 0.625 mm slices reformatted in the axial, coronal and sagittal planes). The right superior semicircular canal was most commonly affected (66.6%). There were 4 bilateral semicircular canal dehiscences. Clinical suspicion of the condition was raised with reliable surrogate history from carers or from older children (100%), a mixed or conductive hearing loss (80% of hearing losses) in the presence of normal impedance audiometry (92.3%), normal transient otoacoustic emissions (84.6%) on the side of the dehiscence and the presence of replicable pathological saccades in the video head impulse test (76.9%). Disequilibrium symptoms and typical third window symptoms were absent or difficult to elicit in children (46.15 and 30.76% respectively). Only 3 (0.5%) fulfilled the adult criteria of a superior semicircular canal dehiscence syndrome. The abnormal video head impulse test characterized by pathological saccades may affect other non-dehisced ipsilateral canals. Semicircular canal dehiscences are rare in children but may be considered as an etiology for hearing losses and imbalance. Children with semicircular canal dehiscence may present differently from the classical superior semicircular canal dehiscence syndrome found in adults.
Keywords: audiovestibular; high resolution CT; pediatric; semicircular canal dehiscence; third window; video head impulse.
Figures
References
-
- Minor LB, Solomon D, Zinreich JS, Zee DS. Sound- and/or pressure-induced vertigo due to bone dehiscence of the superior semicircular canal. Surgery. (1998) 124:249–58. - PubMed
LinkOut - more resources
Full Text Sources