

Cost-effectiveness of Treatment Regimens for Clostridioides difficile Infection: An Evaluation of the 2018 Infectious Diseases Society of America Guidelines
- PMID: 31001619
- PMCID: PMC7319265
- DOI: 10.1093/cid/ciz318
Cost-effectiveness of Treatment Regimens for Clostridioides difficile Infection: An Evaluation of the 2018 Infectious Diseases Society of America Guidelines
Abstract
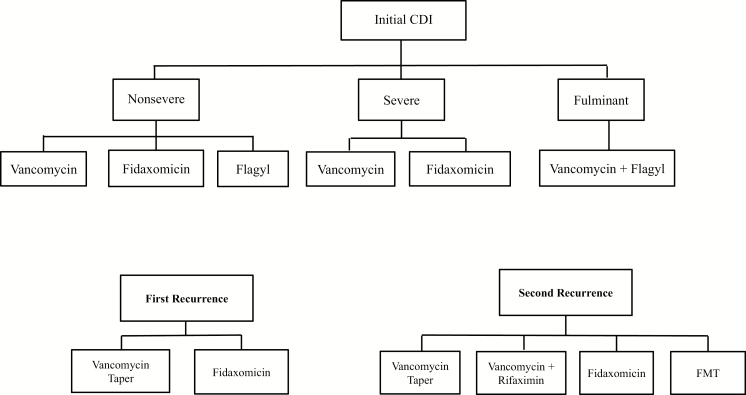
Background: In 2018, the Infectious Diseases Society of America (IDSA) published guidelines for diagnosis and treatment of Clostridioides (formerly Clostridium) difficile infection (CDI). However, there is little guidance regarding which treatments are cost-effective.
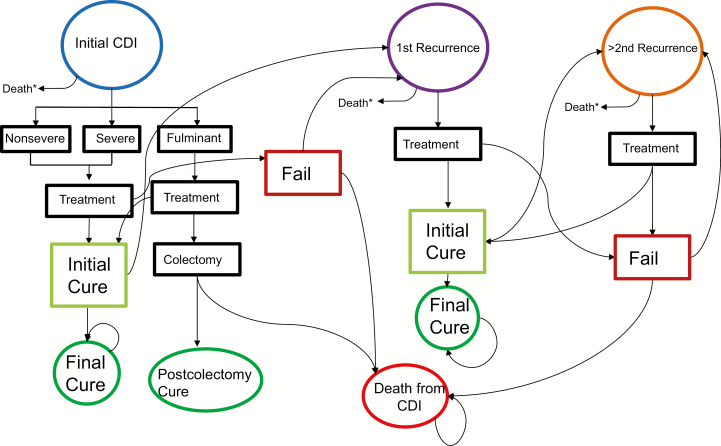
Methods: We used a Markov model to simulate a cohort of patients presenting with an initial CDI diagnosis. We used the model to estimate the costs, effectiveness, and cost-effectiveness of different CDI treatment regimens recommended in the recently published 2018 IDSA guidelines. The model includes stratification by the severity of the initial infection, and subsequent likelihood of cure, recurrence, mortality, and outcomes of subsequent recurrences. Data sources were taken from IDSA guidelines and published literature on treatment outcomes. Outcome measures were discounted quality-adjusted life-years (QALYs), costs, and incremental cost-effectiveness ratios (ICERs).
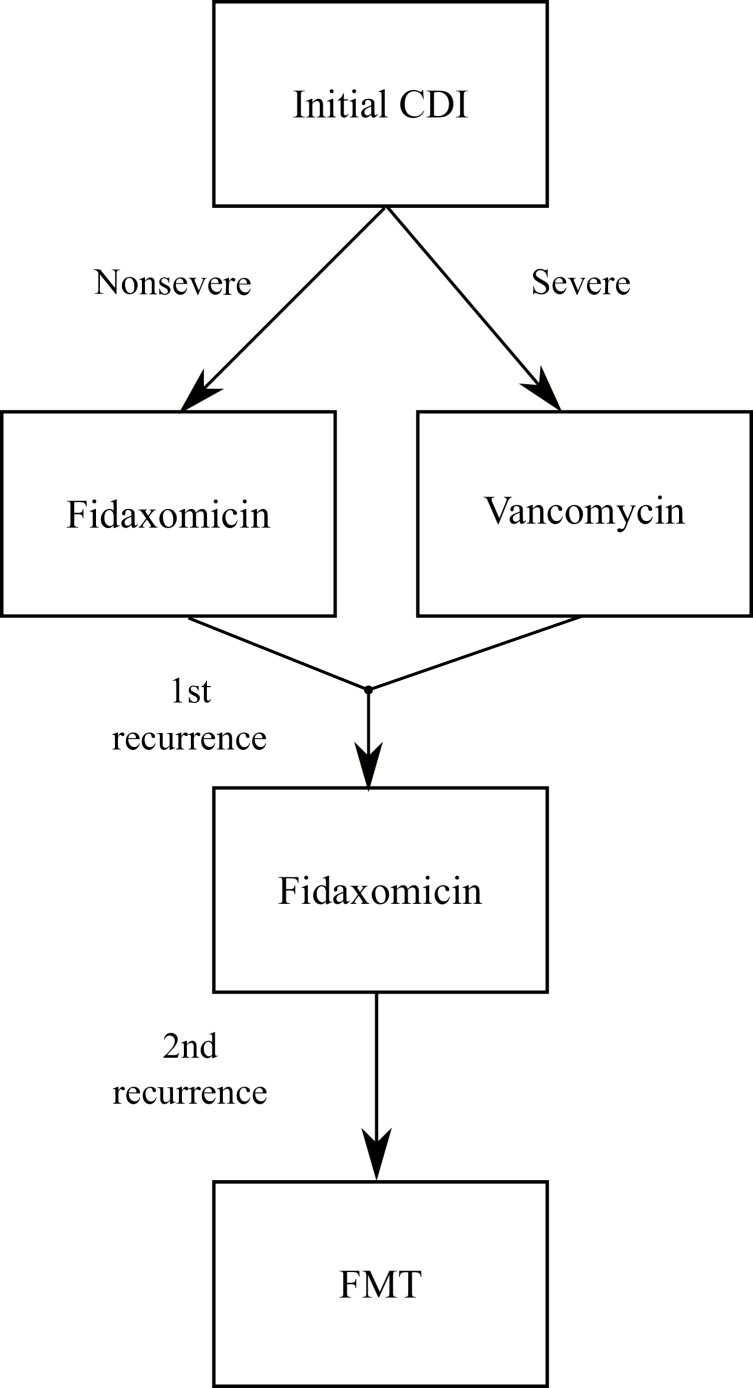
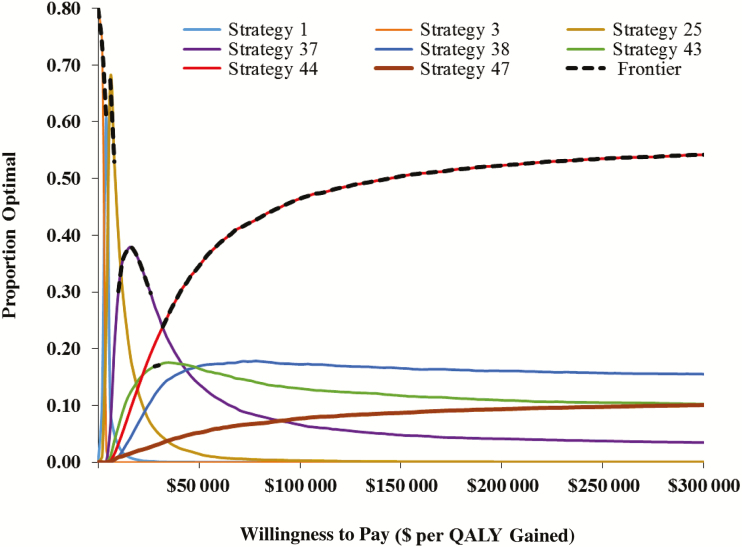
Results: Use of fidaxomicin for nonsevere initial CDI, vancomycin for severe CDI, fidaxomicin for first recurrence, and fecal microbiota transplantation (FMT) for subsequent recurrence (strategy 44) cost an additional $478 for 0.009 QALYs gained per CDI patient, resulting in an ICER of $31 751 per QALY, below the willingness-to-pay threshold of $100 000/QALY. This is the optimal, cost-effective CDI treatment strategy.
Conclusions: Metronidazole is suboptimal for nonsevere CDI as it is less beneficial than alternative strategies. The preferred treatment regimen is fidaxomicin for nonsevere CDI, vancomycin for severe CDI, fidaxomicin for first recurrence, and FMT for subsequent recurrence. The most effective treatments, with highest cure rates, are also cost-effective due to averted mortality, utility loss, and costs of rehospitalization and/or further treatments for recurrent CDI.
Keywords: Clostridioides difficile infection; Clostridium difficile infection; cost-effectiveness.
© The Author(s) 2019. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Reply to Author.Clin Infect Dis. 2022 Feb 11;74(3):563. doi: 10.1093/cid/ciaa740. Clin Infect Dis. 2022. PMID: 32516366 Free PMC article. No abstract available.
-
Cost-Effective Treatment of Clostridiodes difficile Infection.Clin Infect Dis. 2022 Sep 30;75(7):1269. doi: 10.1093/cid/ciac369. Clin Infect Dis. 2022. PMID: 35594558 No abstract available.
References
-
- Ghantoji SS, Sail K, Lairson DR, DuPont HL, Garey KW. Economic healthcare costs of Clostridium difficile infection: a systematic review. J Hosp Infect 2010; 74:309–18. - PubMed
-
- Zimlichman E, Henderson D, Tamir O, et al. Health care-associated infections: a meta-analysis of costs and financial impact on the US health care system. JAMA Intern Med 2013; 173:2039–46. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
