

Comparison of a Potential Hospital Quality Metric With Existing Metrics for Surgical Quality-Associated Readmission
- PMID: 31002316
- PMCID: PMC6481441
- DOI: 10.1001/jamanetworkopen.2019.1313
Comparison of a Potential Hospital Quality Metric With Existing Metrics for Surgical Quality-Associated Readmission
Abstract
Importance: The existing readmission quality metric does not meaningfully distinguish readmissions associated with surgical quality from those that are not associated with surgical quality and thus may not reflect the quality of surgical care.
Objective: To compare a quality metric that classifies readmissions associated with surgical quality with the existing metric of any unplanned readmission in a surgical population.
Design, setting, and participants: Cohort study using US nationwide administrative data collected on 4 high-volume surgical procedures performed at 103 Veterans Affairs hospitals from October 1, 2007, through September 30, 2014. Data analysis was conducted from October 1, 2017, to January 24, 2019.
Main outcomes and measures: Hospital-level rates of unplanned readmission (existing metric) and surgical readmissions associated with surgical quality (new metric) in the 30 days following hospital discharge for an inpatient surgical procedure.
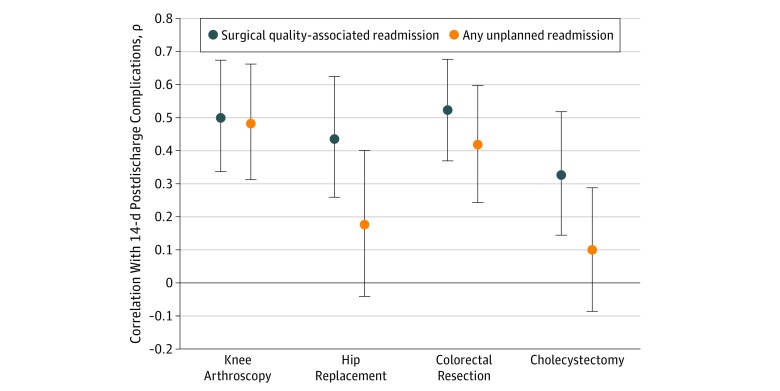
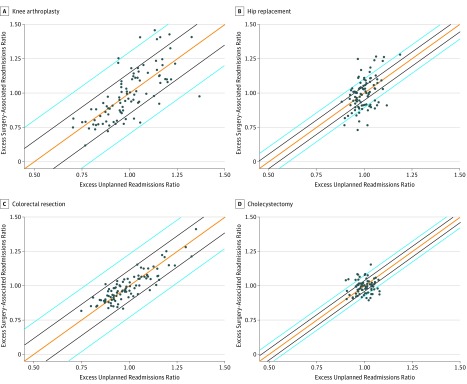
Results: The study population included 109 258 patients who underwent surgery at 103 hospitals. Patients were majority male (94.1%) and white (78.2%) with a mean (SD) age of 64.0 (10.0) years at the time of surgery. After case-mix adjustment, 30-day surgical readmissions ranged from 4.6% (95% CI, 4.5%-4.8%) among knee arthroplasties to 11.1% (95% CI, 10.9%-11.3%) among colorectal resections. The new surgical readmission metric was significantly correlated with facility-level postdischarge complications for all procedures, with ρ coefficients ranging from 0.33 (95% CI, 0.13-0.51) for cholecystectomy to 0.52 (95% CI, 0.38-0.68) for colorectal resection. Correlations between postdischarge complications and the new surgical readmission metric were higher than correlations between complications and the existing readmission metric for all procedures examined (knee arthroplasty: 0.50 vs 0.48; hip replacement: 0.44 vs 0.18; colorectal resection: 0.52 vs 0.42; and cholecystectomy: 0.33 vs 0.10). When compared with using the existing readmission metric, using the new surgical readmission metric could change hip replacement-associated payment penalty determinations in 28.4% of hospitals and knee arthroplasty-associated penalties in 26.0% of hospitals.
Conclusions and relevance: In this study, surgical quality-associated readmissions were more correlated with postdischarge complications at a higher rate than were unplanned readmissions. Thus, a metric based on such readmissions may be a better measure of surgical care quality. This work provides an important step in the development of future value-based payments and promotes evidence-based quality metrics targeting the quality of surgical care.
Conflict of interest statement
Figures
Comment in
-
Clinical Accountability and Measuring Surgical Readmissions.JAMA Netw Open. 2019 Apr 5;2(4):e191301. doi: 10.1001/jamanetworkopen.2019.1301. JAMA Netw Open. 2019. PMID: 31002315 Free PMC article. No abstract available.
Similar articles
-
Comparison of Hospital Readmission After Total Hip and Total Knee Arthroplasty vs Spinal Surgery After Implementation of the Hospital Readmissions Reduction Program.JAMA Netw Open. 2019 May 3;2(5):e194634. doi: 10.1001/jamanetworkopen.2019.4634. JAMA Netw Open. 2019. PMID: 31150074 Free PMC article.
-
Inaugural Readmission Penalties for Total Hip and Total Knee Arthroplasty Procedures Under the Hospital Readmissions Reduction Program.JAMA Netw Open. 2019 Nov 1;2(11):e1916008. doi: 10.1001/jamanetworkopen.2019.16008. JAMA Netw Open. 2019. PMID: 31755949 Free PMC article.
-
Patterns and Costs of 90-Day Readmission for Surgical and Medical Complications Following Total Hip and Knee Arthroplasty.J Arthroplasty. 2019 Oct;34(10):2304-2307. doi: 10.1016/j.arth.2019.05.046. Epub 2019 Jun 1. J Arthroplasty. 2019. PMID: 31279598 Free PMC article.
-
The Validity of All-Cause 30-Day Readmission Rate as a Hospital Performance Metric After Primary Total Hip and Knee Arthroplasty: A Systematic Review.J Arthroplasty. 2019 Aug;34(8):1831-1836. doi: 10.1016/j.arth.2019.04.011. Epub 2019 Apr 13. J Arthroplasty. 2019. PMID: 31072744
-
Towards a patient journey perspective on causes of unplanned readmissions using a classification framework: results of a systematic review with narrative synthesis.BMC Med Res Methodol. 2019 Oct 4;19(1):189. doi: 10.1186/s12874-019-0822-9. BMC Med Res Methodol. 2019. PMID: 31585528 Free PMC article.
Cited by
-
Is Patient Satisfaction Dictated by Quality of Care Among Patients Undergoing Complex Surgical Procedures for a Malignant Indication?Ann Surg Oncol. 2020 Sep;27(9):3126-3135. doi: 10.1245/s10434-020-08788-w. Epub 2020 Jul 7. Ann Surg Oncol. 2020. PMID: 32638162
-
An evaluation of the outcome metric 'days alive and at home' in older patients after hip fracture surgery.Anaesthesia. 2022 Aug;77(8):901-909. doi: 10.1111/anae.15742. Epub 2022 Apr 30. Anaesthesia. 2022. PMID: 35489814 Free PMC article.
-
Comparing textbook outcomes among patients undergoing surgery for cancer at U. S. News & World Report ranked hospitals.J Surg Oncol. 2020 May;121(6):927-935. doi: 10.1002/jso.25833. Epub 2020 Mar 2. J Surg Oncol. 2020. PMID: 32124433 Free PMC article.
-
Private-Sector Readmissions for Inpatient Surgery in Veterans Health Administration Hospitals.JAMA Netw Open. 2024 Dec 2;7(12):e2452056. doi: 10.1001/jamanetworkopen.2024.52056. JAMA Netw Open. 2024. PMID: 39724374 Free PMC article.
-
Prescriptive analytics for reducing 30-day hospital readmissions after general surgery.PLoS One. 2020 Sep 9;15(9):e0238118. doi: 10.1371/journal.pone.0238118. eCollection 2020. PLoS One. 2020. PMID: 32903282 Free PMC article.
References
-
- Centers for Medicare & Medicaid Services All-cause hospital-wide measure updates and specifications report: hospital-level 30-day risk-standardized readmission measure, version 6.0. 2017. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Inst.... Accessed February 25, 2019.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
