

Comparison of Risk of Osteoporotic Fracture in Denosumab vs Alendronate Treatment Within 3 Years of Initiation
- PMID: 31002319
- PMCID: PMC6481596
- DOI: 10.1001/jamanetworkopen.2019.2416
Comparison of Risk of Osteoporotic Fracture in Denosumab vs Alendronate Treatment Within 3 Years of Initiation
Abstract
Importance: Head-to-head randomized clinical trials showed greater efficacy of denosumab vs alendronate in improving bone mineral density. Although there is an association of changes in bone mineral density with reductions in fracture risk, the magnitude of the association is not well established.
Objective: To compare the risk of hip and any fracture in patients treated with denosumab and alendronate in routine practice settings.
Design, setting, and participants: This Danish nationwide, population-based, historical cohort study of a population with universal access to health care used prospectively collected, individually linked data from Danish health registries with complete follow-up. Cohorts consisted of 92 355 individuals 50 years or older who were new users of denosumab (n = 4624) or alendronate (n = 87 731) from May 2010 to December 2017 after at least 1 year without an antiosteoporosis medication dispensing.
Exposures: Initiation of denosumab or alendronate.
Main outcomes and measures: The primary outcome was hospitalization for hip fracture, and the secondary outcome was hospitalization for any fracture. Inverse probability of treatment weights and the intention-to-treat approach were used to calculate cumulative incidences and adjusted hazard ratios (aHRs) with 95% CIs.
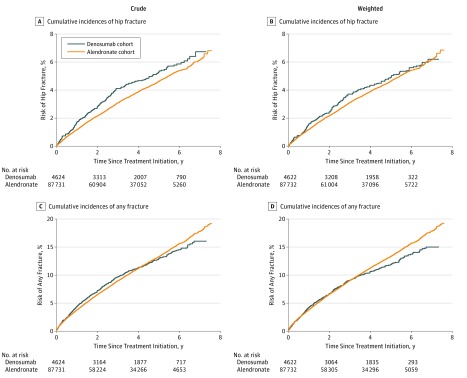
Results: Of the 92 355 included patients, 75 046 (81.3%) were women, and the mean (SD) age was 71 (10) years. The denosumab cohort had a lower proportion of men than the alendronate cohort (12.7% [589] vs 19.0% [16 700]), while age distributions were similar in the 2 cohorts. Within 3 years of follow-up, initiation of denosumab or alendronate was associated with cumulative incidences of 3.7% and 3.1%, respectively, for hip fracture and 9.0% and 9.0%, respectively, for any fracture. Overall, the aHRs for denosumab vs alendronate were 1.08 (95% CI, 0.92-1.28) for hip fracture and 0.92 (95% CI, 0.83-1.02) for any fracture. The aHR of denosumab vs alendronate for hip fracture was 1.07 (95% CI, 0.85-1.34) among patients with a history of any fracture and 1.05 (95% CI, 0.83-1.32) among patients without history of fracture. The aHR for any fracture for denosumab vs alendronate was 0.84 (95% CI, 0.71-0.98) among patients with a history of any fracture and 0.77 (95% CI, 0.64-0.93) among patients with no history of fracture.
Conclusions and relevance: Treatment with denosumab and alendronate was associated with similar risks of hip or any fracture over a 3-year period, regardless of fracture history.
Conflict of interest statement
Figures
Similar articles
-
The Efficacy of Alendronate Versus Denosumab on Major Osteoporotic Fracture Risk in Elderly Patients With Diabetes Mellitus: A Danish Retrospective Cohort Study.Front Endocrinol (Lausanne). 2022 Jan 26;12:826997. doi: 10.3389/fendo.2021.826997. eCollection 2021. Front Endocrinol (Lausanne). 2022. PMID: 35154013 Free PMC article.
-
Comparative effectiveness of denosumab vs alendronate among postmenopausal women with osteoporosis.J Bone Miner Res. 2024 Aug 5;39(7):826-834. doi: 10.1093/jbmr/zjae079. J Bone Miner Res. 2024. PMID: 38753892 Free PMC article.
-
Denosumab and clinical outcomes among men with osteoporosis: a retrospective cohort study.Osteoporos Int. 2025 Mar;36(3):465-473. doi: 10.1007/s00198-024-07381-1. Epub 2025 Jan 8. Osteoporos Int. 2025. PMID: 39777487 Free PMC article.
-
Screening for Osteoporosis to Prevent Fractures: A Systematic Evidence Review for the US Preventive Services Task Force.JAMA. 2025 Feb 11;333(6):509-531. doi: 10.1001/jama.2024.21653. JAMA. 2025. PMID: 39808441
-
Advances in treatment of glucocorticoid-induced osteoporosis.Curr Opin Endocrinol Diabetes Obes. 2017 Dec;24(6):411-417. doi: 10.1097/MED.0000000000000368. Curr Opin Endocrinol Diabetes Obes. 2017. PMID: 28857847 Free PMC article. Review.
Cited by
-
Real-life short-term effectiveness of anti-osteoporotic treatments: a longitudinal cohort study.Ther Adv Musculoskelet Dis. 2022 Jun 27;14:1759720X221105009. doi: 10.1177/1759720X221105009. eCollection 2022. Ther Adv Musculoskelet Dis. 2022. PMID: 35784611 Free PMC article.
-
Hypocalcemia in Patients With Osteoporosis and Normal Renal Function, Treated With Denosumab, a Retrospective Analysis.Nutr Metab Insights. 2024 Jan 8;17:11786388231223604. doi: 10.1177/11786388231223604. eCollection 2024. Nutr Metab Insights. 2024. PMID: 38205220 Free PMC article.
-
Denosumab's Therapeutic Effect for Future Osteosarcopenia Therapy : A Systematic Review and Meta-Analysis.Ann Geriatr Med Res. 2023 Mar;27(1):32-41. doi: 10.4235/agmr.22.0139. Epub 2023 Jan 11. Ann Geriatr Med Res. 2023. Retraction in: Ann Geriatr Med Res. 2023 Dec;27(4):361. doi: 10.4235/agmr.22.0139.r1. PMID: 36628511 Free PMC article. Retracted.
-
Is the Jaw Bone Micro-Structure Altered in Response to Osteoporosis and Bisphosphonate Treatment? A Micro-CT Analysis.Int J Mol Sci. 2021 Jun 18;22(12):6559. doi: 10.3390/ijms22126559. Int J Mol Sci. 2021. PMID: 34207275 Free PMC article.
-
Postoperative Administration of the Acetylcholinesterase Inhibitor, Donepezil, Interferes with Bone Healing and Implant Osseointegration in a Rat Model.Biomolecules. 2020 Sep 14;10(9):1318. doi: 10.3390/biom10091318. Biomolecules. 2020. PMID: 32937955 Free PMC article.
References
-
- Hernlund E, Svedbom A, Ivergård M, et al. . Osteoporosis in the European Union: medical management, epidemiology and economic burden: a report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch Osteoporos. 2013;8(1-2):136. doi:10.1007/s11657-013-0136-1 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
