

SMFM Special Statement: State of the science on multifetal gestations: unique considerations and importance
- PMID: 31002766
- PMCID: PMC7556908
- DOI: 10.1016/j.ajog.2019.04.013
SMFM Special Statement: State of the science on multifetal gestations: unique considerations and importance
Abstract
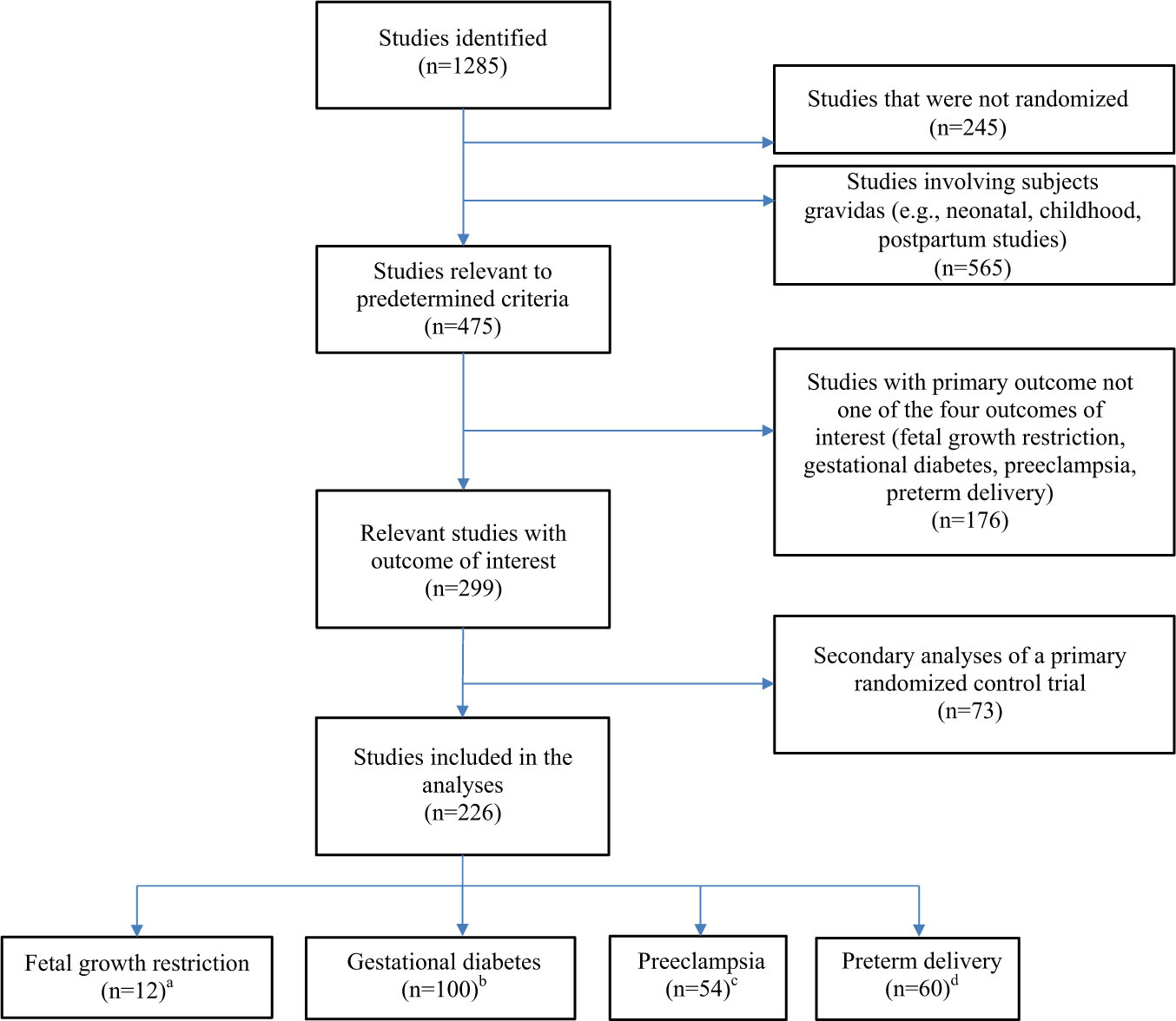
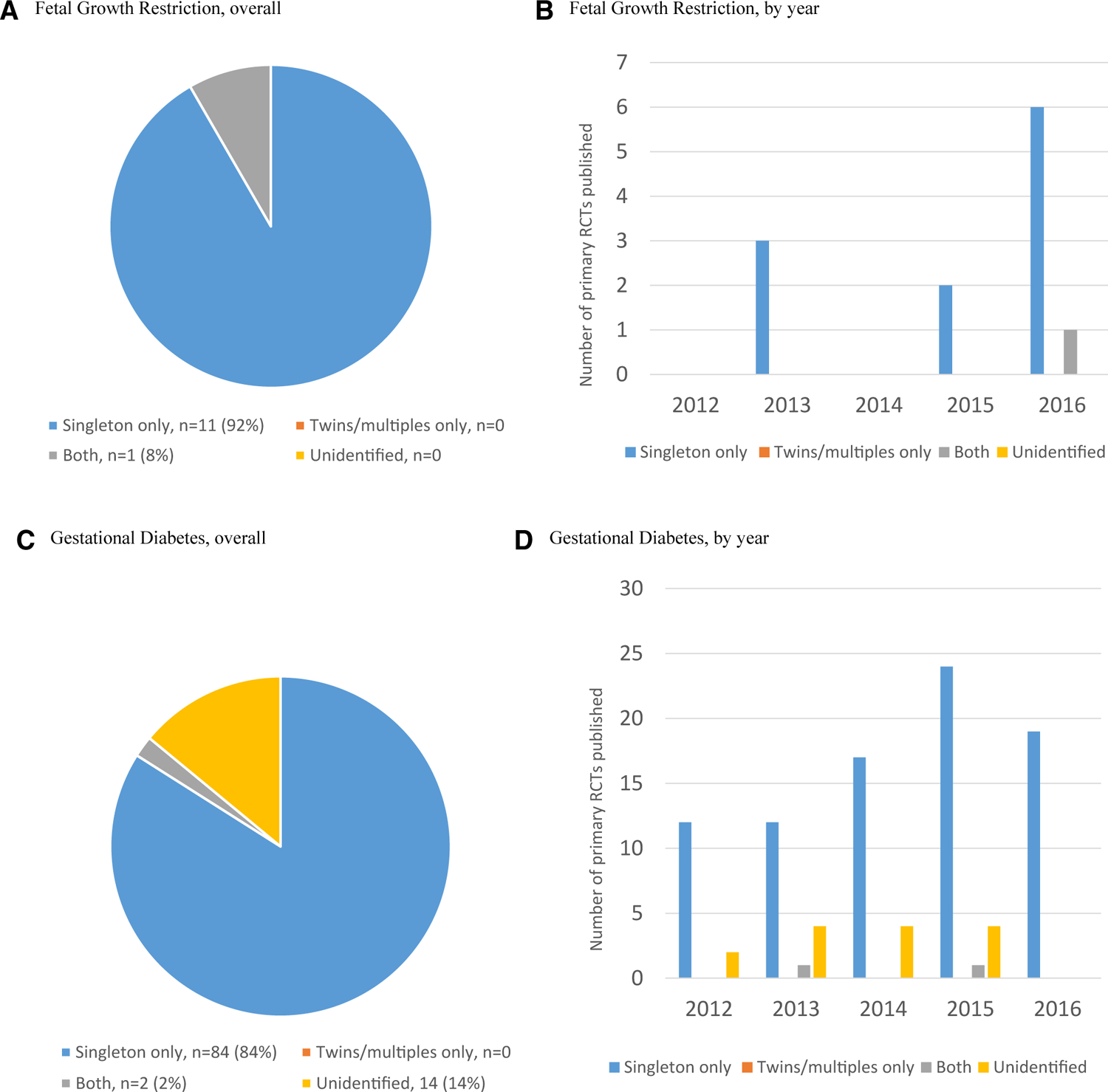
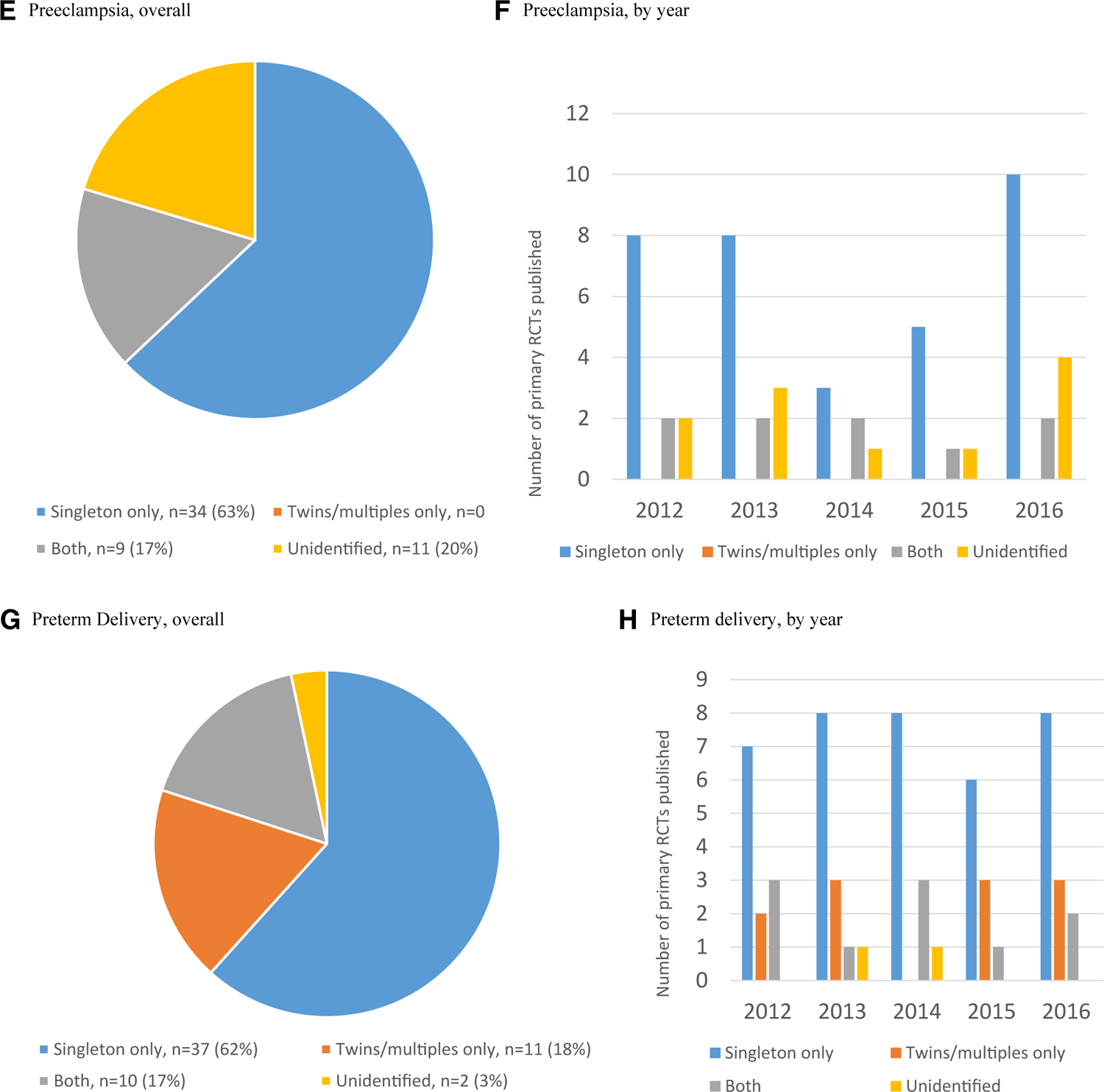
We sought to review the state of the science for research on multiple gestations. A literature search was performed with the use of PubMed for studies to quantify the representation of multiple gestations for a sample period (2012-2016) that were limited to phase III and IV randomized controlled trials, that were written in English, and that addressed at least 1 of 4 major pregnancy complications: fetal growth restriction or small-for-gestational-age fetus, gestational diabetes mellitus, preeclampsia, and preterm delivery. Of the 226 studies that are included in the analysis, multiple pregnancies were most represented in studies of preterm delivery: 17% of trials recruited both singleton and multiple pregnancies; another 18% of trials recruited only multiple pregnancies. For trials that studied preeclampsia, fetal growth restriction, and gestational diabetes mellitus, 17%, 8%, and 2%, respectively, recruited both singleton and multiple gestations. None of the trials on these 3 topics were limited to women with a multiple pregnancy. Women with a multiple pregnancy are at risk for complications similar to those of women with singleton pregnancies, but their risk is usually higher. Also, the pathophysiologic condition for some complications differs in multiple gestations from those that occur in singleton gestations. Conditions that are unique to multiple pregnancies include excess placenta, placental crowding or inability of the uteroplacental unit to support the normal growth of multiple fetuses, or suboptimal placental implantation sites with an increased risk of abnormal placental location. Other adverse outcomes in multiple gestations are also influenced by twin-specific risk factors, most notably chorionicity. Although twins have been well represented in many studies of preterm birth, these studies have failed to identify adequate predictive tests (short cervical length established over 2 decades ago remains the single best predictor), to establish effective interventions, and to differentiate the underlying pathophysiologic condition of twin preterm birth. Questions about fetal growth also remain. Twin growth deviates from that of singleton gestations starting at approximately 32 weeks of gestation; however, research with long-term follow-up is needed to better distinguish pathologic and physiologic growth deviations, which include growth discordance among pairs (or more). There are virtually no clinical trials that are specific to twins for gestational diabetes mellitus or preeclampsia, and subgroups for multiple pregnancies in existing trials are not large enough to allow definite conclusions. Another important area is the determination of appropriate maternal nutrition or micronutrient supplementation to optimize pregnancy and child health. There are also unique aspects to consider for research design in multiple gestations, such as designation and tracking of the correct fetus prenatally and through delivery. The correct statistical methods must be used to account for correlated data because multiple fetuses share the same mother and intrauterine environment. In summary, multiple gestations often are excluded from research studies, despite a disproportionate contribution to national rates of perinatal morbidity, mortality, and health-care costs. It is important to consider the enrollment of multifetal pregnancies in studies that target mainly women with singleton gestations, even when sample size is inadequate, so that insights that are specific to multiple gestations can be obtained when results of smaller studies are pooled together. The care of pregnant women with multiple gestations presents unique challenges; unfortunately, evidence-based clinical management that includes the diagnosis and treatment of common obstetrics problems are not well-defined for this population.
Copyright © 2019. Published by Elsevier Inc.
Conflict of interest statement
The remaining authors report no conflict of interest.
Figures
References
-
- Martin JA, Hamilton BE, Osterman MJK, Driscoll AK, Drake P. Births: final data for 2016. Natl Vital Stat Rep 2018;67:1–55. - PubMed
-
- Blondel B, Kaminski M. Trends in the occurrence, determinants, and consequences of multiple births. Semin Perinatol 2002;26:239–49. - PubMed
-
- Adashi EY, Gutman R. Delayed childbearing as a growing, previously unrecognized contributor to the national plural birth excess. Obstet Gynecol 2018;132:999–1006. - PubMed
-
- Stern JE, Cedars MI, Jain T, et al. Assisted reproductive technology practice patterns and the impact of embryo transfer guidelines in the United States. Fertil Steril 2007;88:275–82. - PubMed
-
- Stulberg DB, Jackson RA, Freedman LR. Referrals for services prohibited in Catholic health care facilities. Perspect Sex Reprod Health 2016;48:111–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
