

Short-Term Effects of Anodal Transcranial Direct Current Stimulation on Endurance and Maximal Force Production. A Systematic Review and Meta-Analysis
- PMID: 31003550
- PMCID: PMC6518246
- DOI: 10.3390/jcm8040536
Short-Term Effects of Anodal Transcranial Direct Current Stimulation on Endurance and Maximal Force Production. A Systematic Review and Meta-Analysis
Abstract
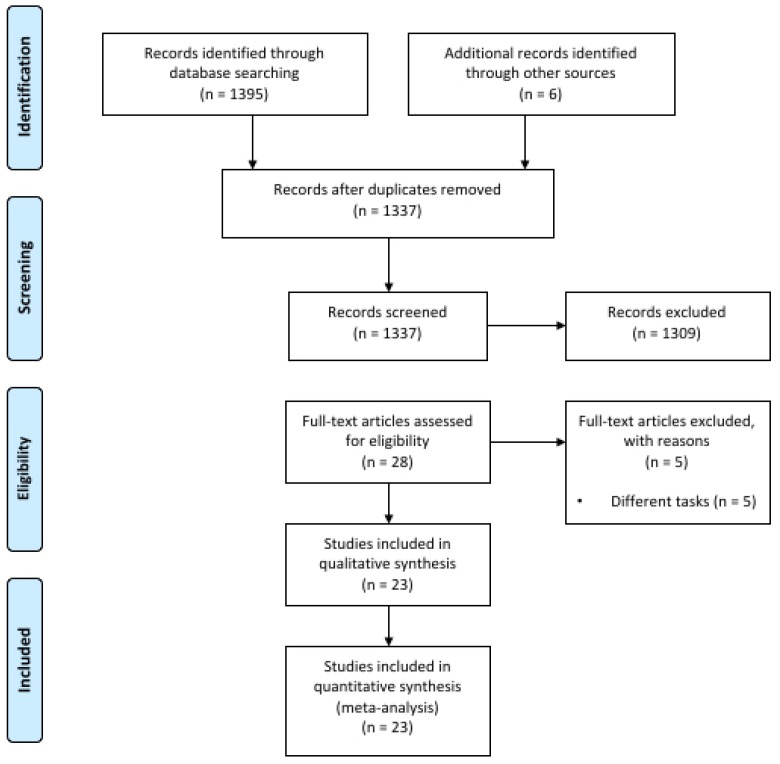
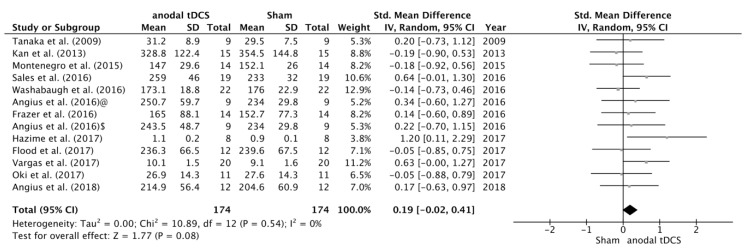
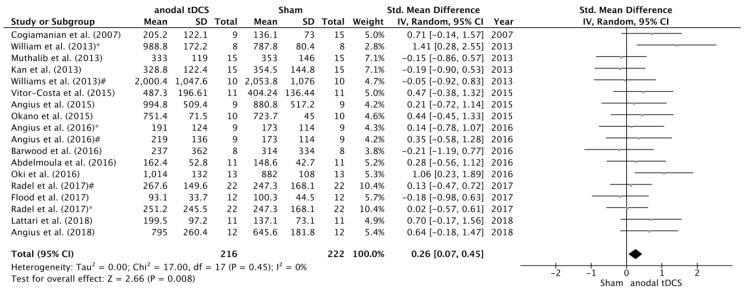
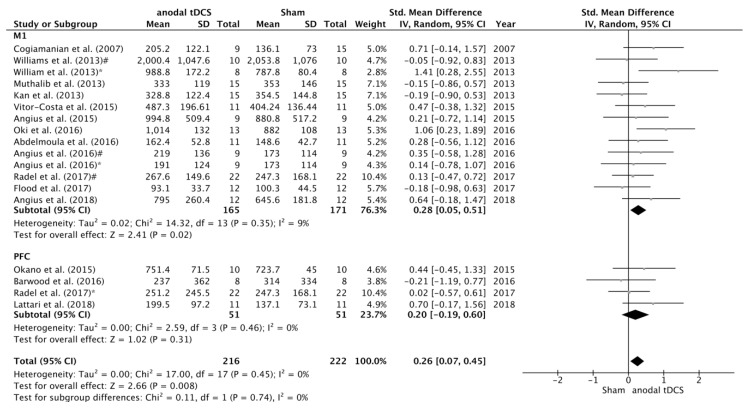
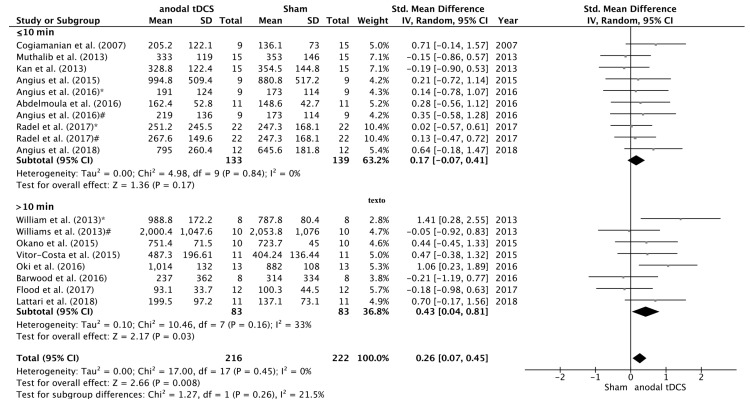
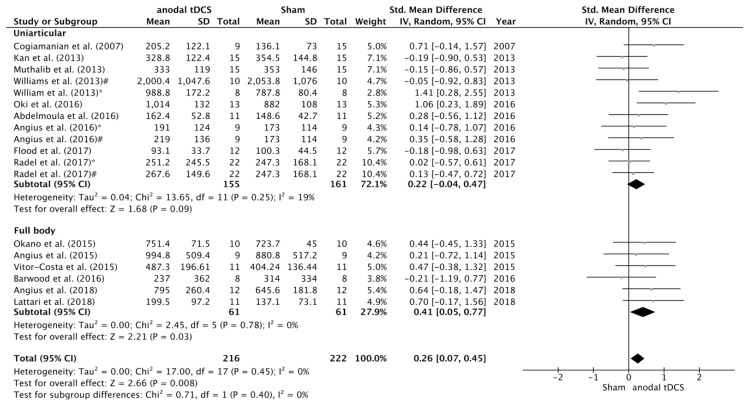
The purpose of the present systematic review and meta-analysis was to explore the effects of transcranial direct current stimulation (tDCS) on endurance (i.e., time to task failure (TTF)) and maximal voluntary contraction (MVC). Furthermore, we aimed to analyze whether the duration of stimulation, the brain region targeted for stimulation, and the task performed could also influence motor performance. We performed a systematic literature review in the databases MEDLINE and Web of Science. The short-term effects of anodal tDCS and sham stimulation (placebo) were considered as experimental and control conditions, respectively. A total of 31 interventions were included (MVC = 13; TTF = 18). Analysis of the strength-related tDCS studies showed small improvements in the MVC (SMD = 0.19; 95% CI = -0.02, 0.41; p = 0.08). However, the results of the endurance-related interventions indicated a moderate effect on TTF performance (SMD = 0.26; 95% CI = 0.07, 0.45; p = 0.008). Furthermore, the sub-analysis showed that anodal tDCS over M1 and stimulation durations longer than 10 min produced the best results in terms of TTF performance enhancement. Additionally, the effects of anodal tDCS were larger during full body exercises (i.e., cycling) when compared to uniarticular tasks. In conclusion, the current meta-analysis indicated that anodal tDCS leads to small and moderate effects on MVC and TTF, respectively.
Keywords: Non-invasive brain stimulation; maximal voluntary contraction; prefrontal cortex; primary motor cortex; time to task failure.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Nitsche M.A., Fricke K., Henschke U., Schlitterlau A., Liebetanz D., Lang N., Henning S., Tergau F., Paulus W. Pharmacological modulation of cortical excitability shifts induced by transcranial direct current stimulation in humans. J. Physiol. 2003;553:293–301. doi: 10.1113/jphysiol.2003.049916. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
