

Diagnosing and quantifying a common deficit in multiple sclerosis: Internuclear ophthalmoplegia
- PMID: 31004067
- PMCID: PMC6598816
- DOI: 10.1212/WNL.0000000000007499
Diagnosing and quantifying a common deficit in multiple sclerosis: Internuclear ophthalmoplegia
Abstract
Objective: We present an objective and quantitative approach for diagnosing internuclear ophthalmoplegia (INO) in multiple sclerosis (MS).
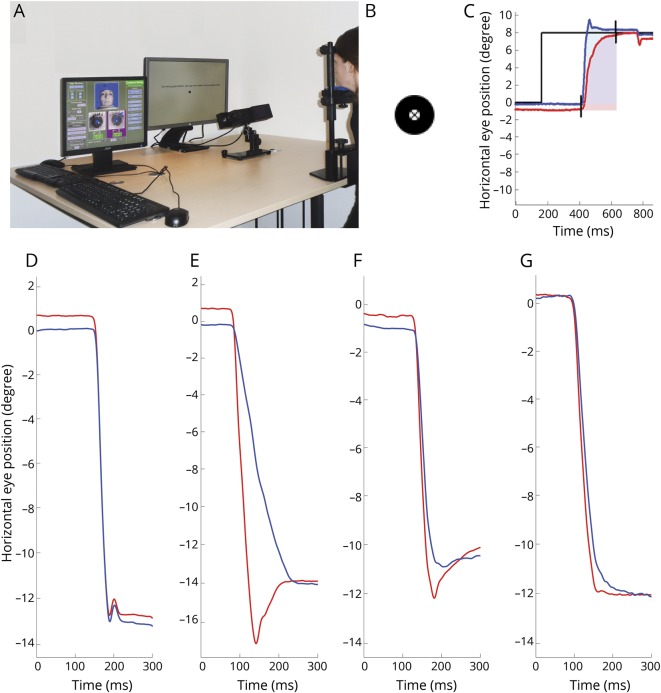
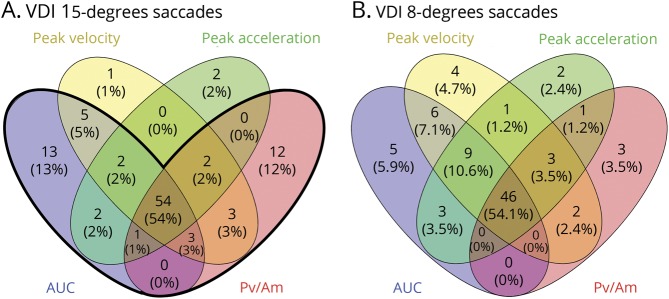
Methods: A validated standardized infrared oculography protocol (DEMoNS [Demonstrate Eye Movement Networks with Saccades]) was used for quantifying prosaccades in patients with MS and healthy controls (HCs). The versional dysconjugacy index (VDI) was calculated, which describes the ratio between the abducting and adducting eye. The VDI was determined for peak velocity, peak acceleration, peak velocity divided by amplitude, and area under the curve (AUC) of the saccadic trajectory. We calculated the diagnostic accuracy for the several VDI parameters by a receiver operating characteristic analysis comparing HCs and patients with MS. The National Eye Institute Visual Function Questionnaire-25 was used to investigate vision-related quality of life of MS patients with INO.
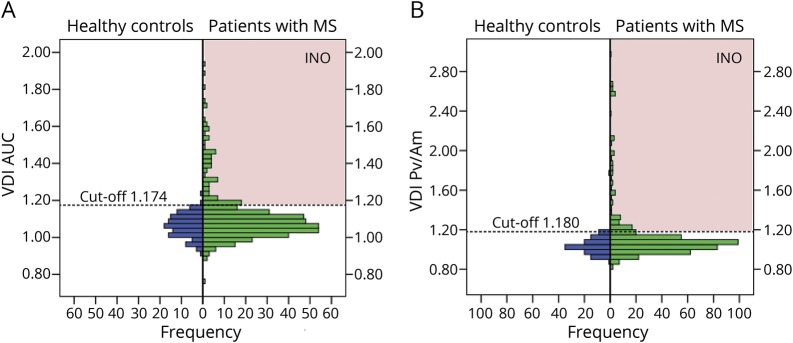
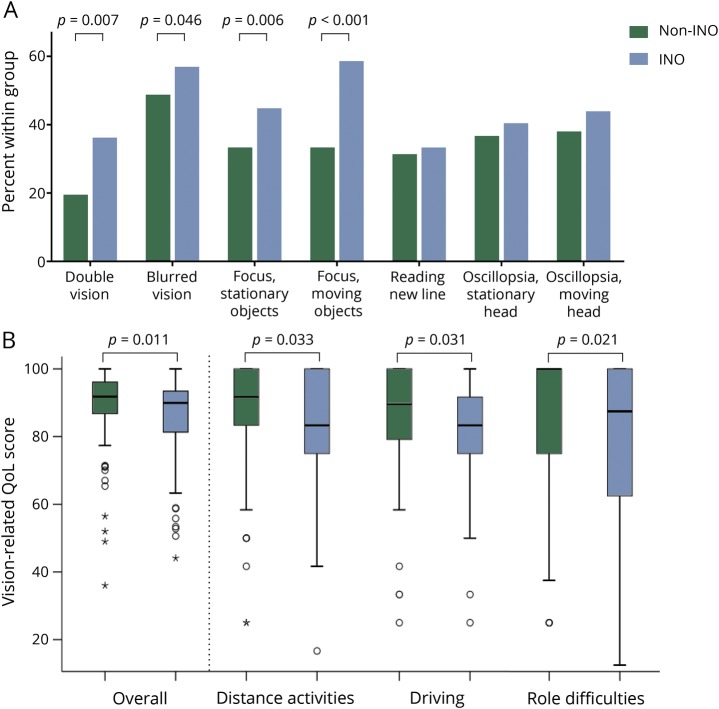
Results: Two hundred ten patients with MS and 58 HCs were included. The highest diagnostic accuracy was achieved by the VDI AUC of 15° horizontal prosaccades. Based on a combined VDI AUC and peak velocity divided by amplitude detection, the prevalence of an INO in MS calculated to 34%. In the INO group, 35.2% of the patients with MS reported any complaints of double vision, compared to 18.4% in the non-INO group (p = 0.010). MS patients with an INO had a lower overall vision-related quality of life (median 89.9, interquartile range 12.8) compared to patients without an INO (median 91.8, interquartile range 9.3, p = 0.011).
Conclusions: This study provides an accurate quantitative and clinically relevant definition of an INO in MS. This infrared oculography-based INO standard will require prospective validation. The high prevalence of INO in MS provides an anatomically well described and accurately quantifiable model for treatment trials in MS.
Copyright © 2019 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
Comment in
-
Personalizing medical care for patients with MS: Monitoring brainstem damage by infrared oculography.Neurology. 2019 May 14;92(20):929-930. doi: 10.1212/WNL.0000000000007493. Epub 2019 Apr 19. Neurology. 2019. PMID: 31004068 No abstract available.
Similar articles
-
A new measure of dysconjugacy in INO: the first-pass amplitude.J Neurol Sci. 2003 Jun 15;210(1-2):65-71. doi: 10.1016/s0022-510x(03)00027-3. J Neurol Sci. 2003. PMID: 12736091
-
Quantitative oculographic characterisation of internuclear ophthalmoparesis in multiple sclerosis: the versional dysconjugacy index Z score.J Neurol Neurosurg Psychiatry. 2002 Jul;73(1):51-5. doi: 10.1136/jnnp.73.1.51. J Neurol Neurosurg Psychiatry. 2002. PMID: 12082045 Free PMC article.
-
The prevalence of internuclear ophthalmoparesis in a population-based cohort of individuals with multiple sclerosis.Mult Scler Relat Disord. 2022 Jul;63:103824. doi: 10.1016/j.msard.2022.103824. Epub 2022 Apr 25. Mult Scler Relat Disord. 2022. PMID: 35490450
-
Ocular Motor Manifestations of Multiple Sclerosis.J Neuroophthalmol. 2017 Sep;37(3):332-340. doi: 10.1097/WNO.0000000000000507. J Neuroophthalmol. 2017. PMID: 28410279 Review.
-
Wall-eyed bilateral internuclear ophthalmoplegia: review of pathogenesis, diagnosis, prognosis and management.Clin Exp Optom. 2015 Jan;98(1):25-30. doi: 10.1111/cxo.12200. Epub 2014 Oct 12. Clin Exp Optom. 2015. PMID: 25308307 Review.
Cited by
-
[Enhancing monitoring of disease progression-remote sensoring in multiple sclerosis].Nervenarzt. 2019 Dec;90(12):1239-1244. doi: 10.1007/s00115-019-00817-8. Nervenarzt. 2019. PMID: 31641794 Review. German.
-
Retinal inter-eye difference and atrophy progression in multiple sclerosis diagnostics.J Neurol Neurosurg Psychiatry. 2022 Feb;93(2):216-219. doi: 10.1136/jnnp-2021-327468. Epub 2021 Nov 11. J Neurol Neurosurg Psychiatry. 2022. PMID: 34764152 Free PMC article.
-
Visuo-Cognitive Phenotypes in Early Multiple Sclerosis: A Multisystem Model of Visual Processing.J Clin Med. 2024 Jan 23;13(3):649. doi: 10.3390/jcm13030649. J Clin Med. 2024. PMID: 38337342 Free PMC article.
-
Eye Movement Evaluation in Multiple Sclerosis and Parkinson's Disease Using a Standardized Oculomotor and Neuro-Ophthalmic Disorder Assessment (SONDA).Front Neurol. 2020 Sep 8;11:971. doi: 10.3389/fneur.2020.00971. eCollection 2020. Front Neurol. 2020. PMID: 33013643 Free PMC article.
-
A model for interrogating the clinico-radiological paradox in multiple sclerosis: Internuclear ophthalmoplegia.Eur J Neurol. 2021 May;28(5):1617-1626. doi: 10.1111/ene.14723. Epub 2021 Feb 8. Eur J Neurol. 2021. PMID: 33426786 Free PMC article.
References
-
- Frohman TC, Frohman EM, O'Suilleabhain P, et al. . Accuracy of clinical detection of INO in MS: corroboration with quantitative infrared oculography. Neurology 2003;61:848–850. - PubMed
-
- Ventre J, Vighetto A, Bailly G, Prablanc C. Saccade metrics in multiple sclerosis: versional velocity disconjugacy as the best clue? J Neurol Sci 1991;102:144–149. - PubMed
-
- Flipse JP, Straathof CSM, van der Steen J, et al. . Binocular saccadic eye movements in multiple sclerosis. J Neurol Sci 1997;148:53–65. - PubMed
-
- Frohman EM, O'Suilleabhain P, Dewey RB, Frohman TC, Kramer PD. A new measure of dysconjugacy in INO: the first-pass amplitude. J Neurol Sci 2003;210:65–71. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical