

[68Ga]Pentixafor PET/MR imaging of chemokine receptor 4 expression in the human carotid artery
- PMID: 31004184
- PMCID: PMC6584241
- DOI: 10.1007/s00259-019-04322-7
[68Ga]Pentixafor PET/MR imaging of chemokine receptor 4 expression in the human carotid artery
Abstract
Purpose: Type 4 chemokine receptor (CXCR4) plays an important role in immune cell migration during the atherosclerosis progression. We aimed to evaluate [68Ga]Pentixafor positron emission tomography (PET) in combination magnetic resonance imaging (MRI) for in vivo quantification of CXCR4 expression in carotid plaques.
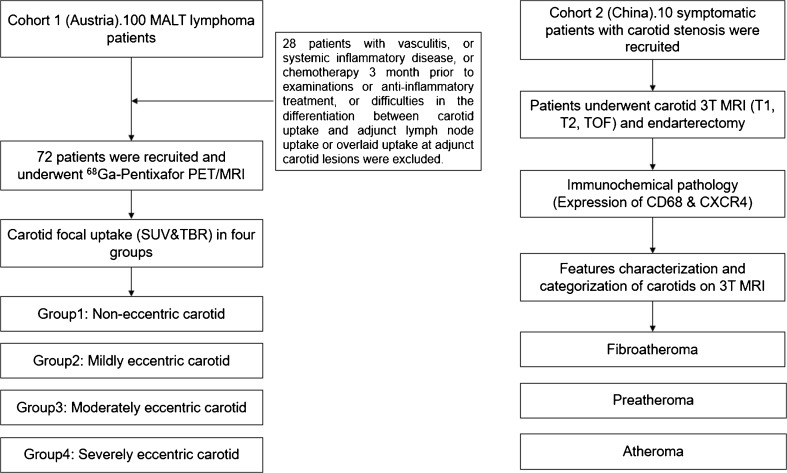
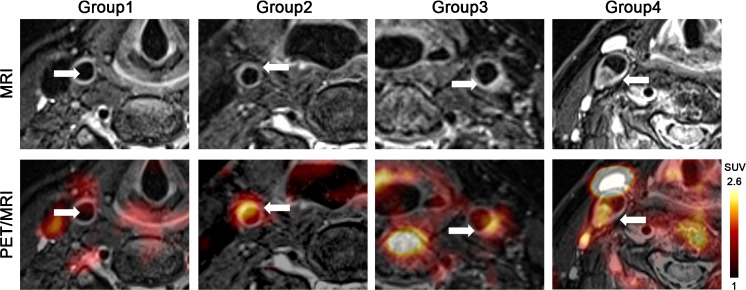
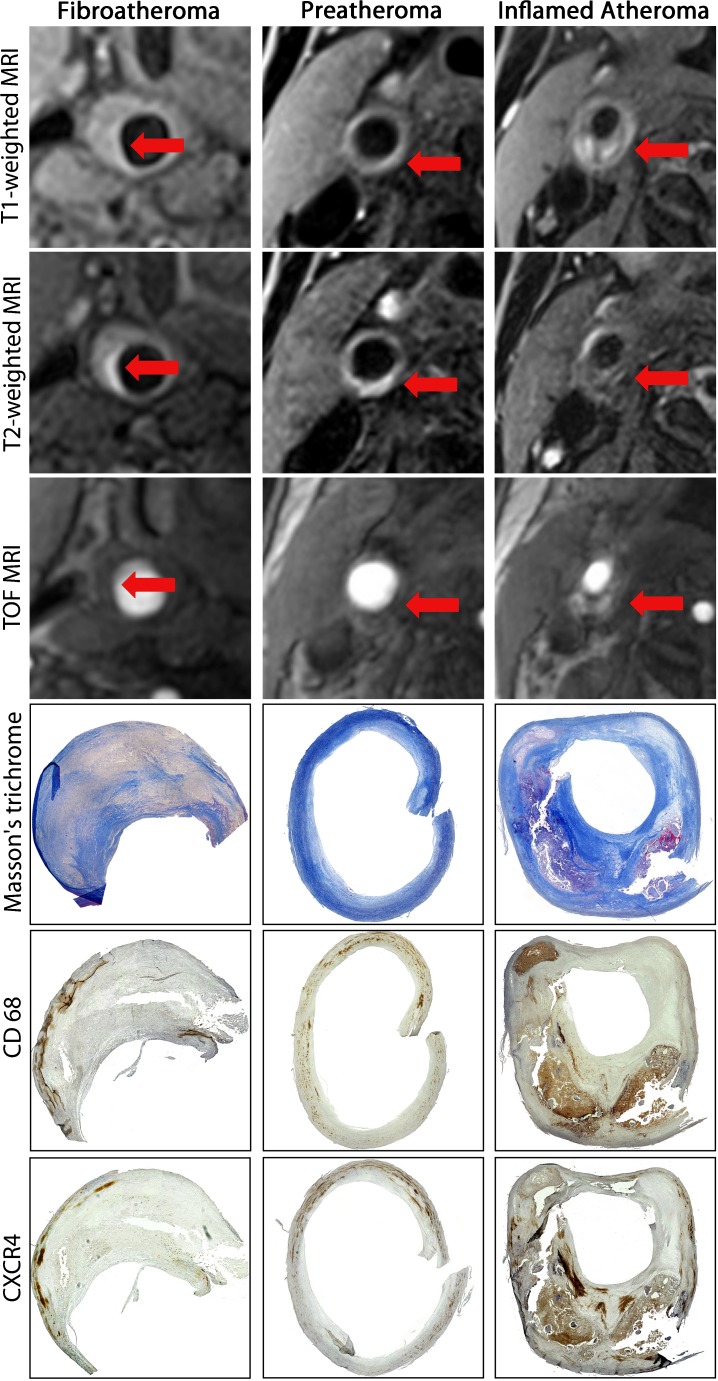
Methods: Seventy-two patients with lymphoma were prospectively scheduled for whole body [68Ga]Pentixafor PET/MRI with an additional T2-weighted carotid sequence. Volumes of interest (VOIs) were drawn along the carotid bifurcation regions, and the maximum tissue-to-blood ratios (TBR) of [68Ga]Pentixafor uptake were calculated. Lesions were categorized into non-eccentric (n = 27), mild eccentric (n = 67), moderately (n = 41) and severely (n = 19) eccentric carotid atherosclerosis. A different cohort of symptomatic patients (n = 10) with carotid stenosis scheduled for thrombendarterectomy (TEA) was separately imaged with 3T MRI with dedicated plaque sequences (time of flight, T1-, and T2-weighted). MRI findings were correlated with histochemical assessment of intact carotid plaques.
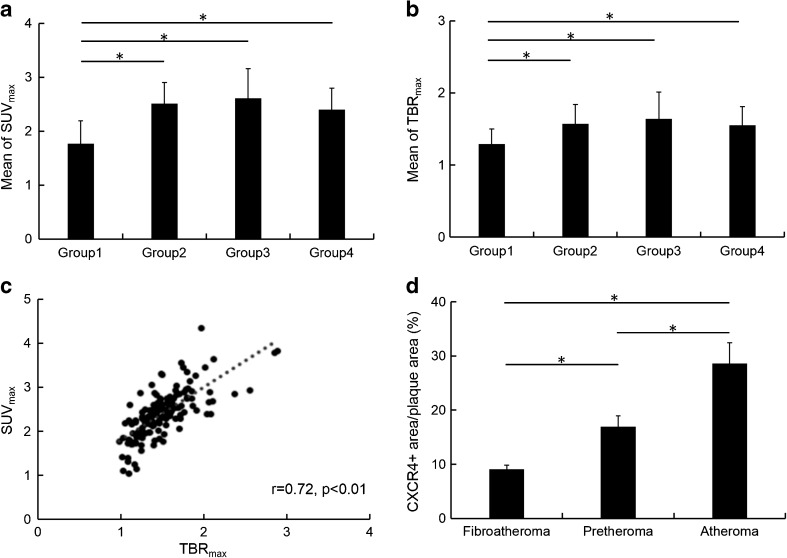
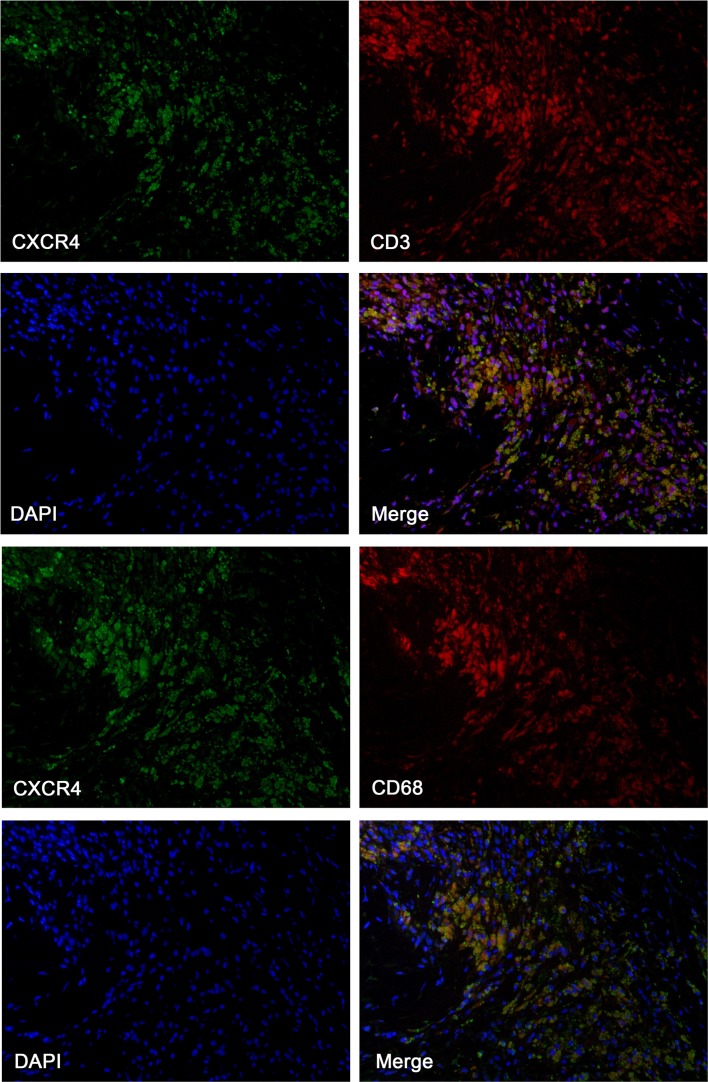
Results: At hybrid PET/MRI, we observed significantly increased [68Ga]Pentixafor uptake in mildly (mean TBRmax = 1.57 ± 0.27, mean SUVmax = 2.51 ± 0.39), moderately (mean TBRmax = 1.64 ± 0.37, mean SUVmax = 2.61 ± 0.55) and severely eccentric carotids (mean TBRmax = 1.55 ± 0.26, mean SUVmax = 2.40 ± 0.44) as compared to non-eccentric carotids (mean TBRmax = 1.29 ± 0.21, mean SUVmax = 1.77 ± 0.42) (p ≤ 0.05). Histological findings from TEA confirmed that prominent CXCR4 expression was localized within inflamed atheromas and preatheromas. Co-localization of cellular CXCR4 and CD68 expression in the plaque was observed by immunofluorescence staining.
Conclusions: In vivo evaluation of CXCR4 expression in carotid atherosclerotic lesions is feasible using [68Ga]Pentixafor PET/MRI. In atherosclerotic plaque tissue, CXCR4 expression might be used as a surrogate marker for inflammatory atherosclerosis.
Keywords: Atherosclerosis; CXCR4; Carotid artery; PET/MRI; [68Ga]Pentixafor.
Conflict of interest statement
Hans-Jürgen Wester is shareholder of SCINTOMICS GmbH, Germany. SCINTOMICS owns the IP on Pentixafor.
The other enlisted authors have no conflict of interest to declare.
Figures
Similar articles
-
[68Ga]Pentixafor-PET/MRI for the detection of Chemokine receptor 4 expression in atherosclerotic plaques.Eur J Nucl Med Mol Imaging. 2018 Apr;45(4):558-566. doi: 10.1007/s00259-017-3831-0. Epub 2017 Sep 21. Eur J Nucl Med Mol Imaging. 2018. PMID: 28932900 Free PMC article.
-
Imaging the Cytokine Receptor CXCR4 in Atherosclerotic Plaques with the Radiotracer 68Ga-Pentixafor for PET.J Nucl Med. 2017 Mar;58(3):499-506. doi: 10.2967/jnumed.116.179663. Epub 2016 Oct 27. J Nucl Med. 2017. PMID: 27789718
-
Prospective non-invasive evaluation of CXCR4 expression for the diagnosis of MALT lymphoma using [68Ga]Ga-Pentixafor-PET/MRI.Theranostics. 2019 May 27;9(12):3653-3658. doi: 10.7150/thno.31032. eCollection 2019. Theranostics. 2019. PMID: 31281504 Free PMC article.
-
Imaging findings and clinical relevance of 68Ga-Pentixafor PET in atherosclerosis: a systematic review.BMC Med Imaging. 2023 Oct 26;23(1):166. doi: 10.1186/s12880-023-01134-y. BMC Med Imaging. 2023. PMID: 37884885 Free PMC article.
-
Advances in PET Imaging of the CXCR4 Receptor: [68Ga]Ga-PentixaFor.Semin Nucl Med. 2024 Jan;54(1):163-170. doi: 10.1053/j.semnuclmed.2023.09.002. Epub 2023 Nov 3. Semin Nucl Med. 2024. PMID: 37923671 Free PMC article. Review.
Cited by
-
Advances in Radiopharmaceutical Sciences for Vascular Inflammation Imaging: Focus on Clinical Applications.Molecules. 2021 Nov 24;26(23):7111. doi: 10.3390/molecules26237111. Molecules. 2021. PMID: 34885690 Free PMC article. Review.
-
Macrophage PET imaging in mouse models of cardiovascular disease and cancer with an apolipoprotein-inspired radiotracer.Npj Imaging. 2024;2(1):12. doi: 10.1038/s44303-024-00009-3. Epub 2024 May 15. Npj Imaging. 2024. PMID: 38765879 Free PMC article.
-
Imaging Carotid Plaque Inflammation Using Positron Emission Tomography: Emerging Role in Clinical Stroke Care, Research Applications, and Future Directions.Cells. 2023 Aug 15;12(16):2073. doi: 10.3390/cells12162073. Cells. 2023. PMID: 37626883 Free PMC article. Review.
-
A new class of PentixaFor- and PentixaTher-based theranostic agents with enhanced CXCR4-targeting efficiency.Theranostics. 2020 Jul 9;10(18):8264-8280. doi: 10.7150/thno.45537. eCollection 2020. Theranostics. 2020. PMID: 32724470 Free PMC article.
-
Left Ventricular Remodelling Associated with the Transient Elevated [68Ga]Ga-Pentixafor Activity in the Remote Myocardium Following Acute Myocardial Infarction.Mol Imaging Biol. 2024 Aug;26(4):693-703. doi: 10.1007/s11307-024-01912-2. Epub 2024 Apr 19. Mol Imaging Biol. 2024. PMID: 38641708
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
