

Background parenchymal enhancement on breast MRI: A comprehensive review
- PMID: 31004391
- PMCID: PMC7207072
- DOI: 10.1002/jmri.26762
Background parenchymal enhancement on breast MRI: A comprehensive review
Abstract
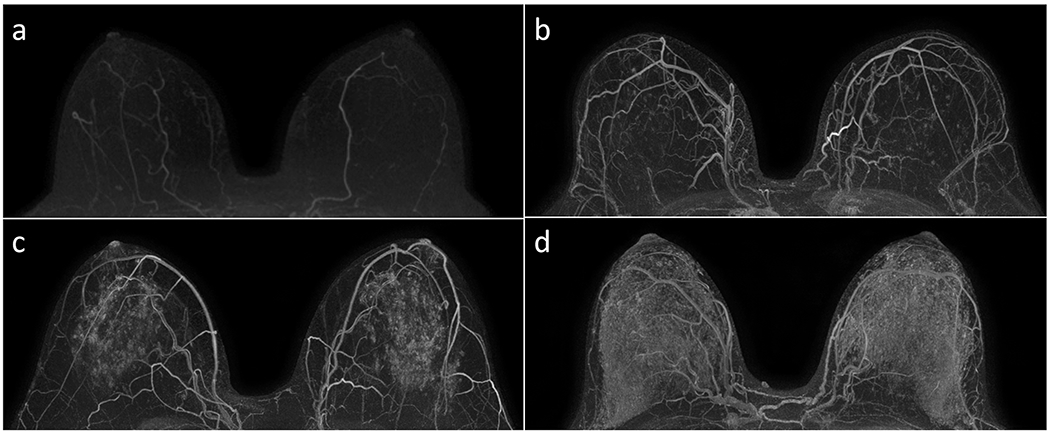
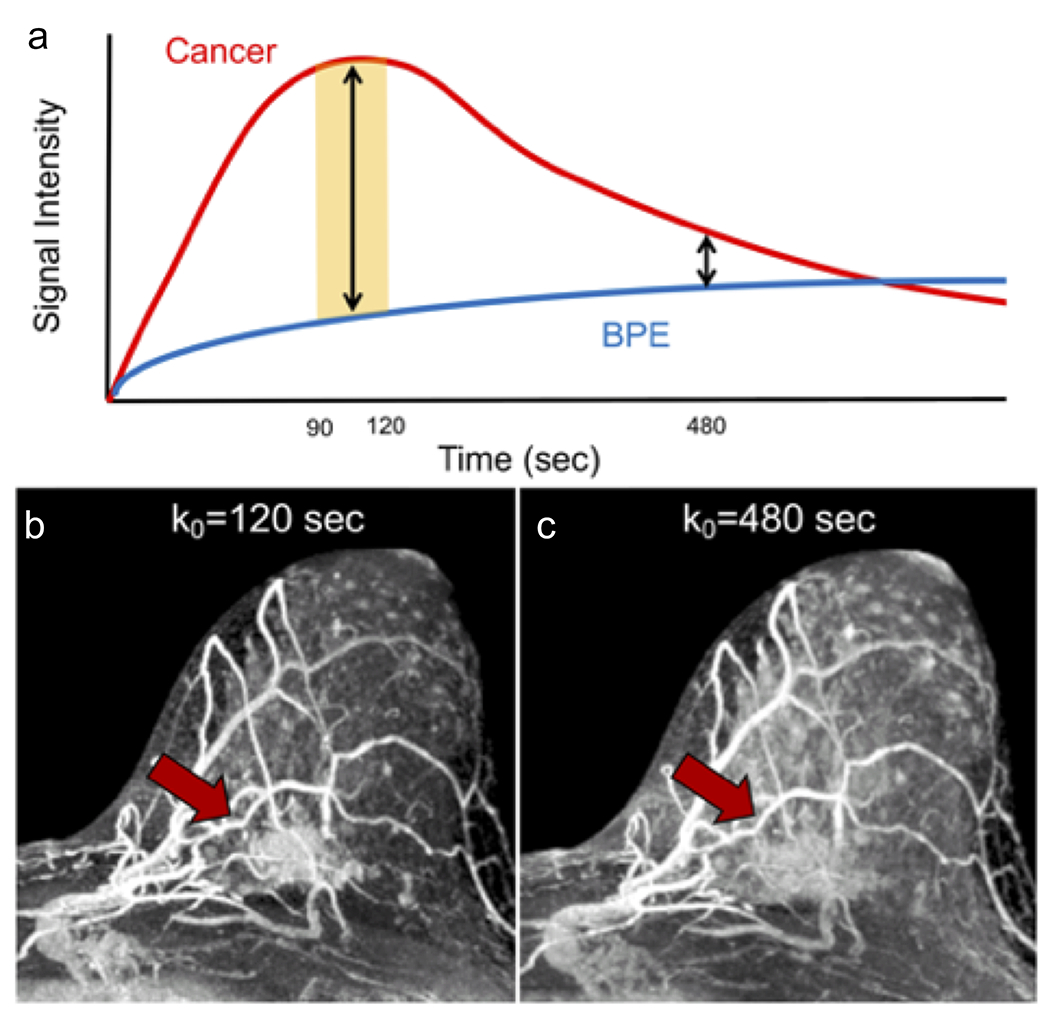
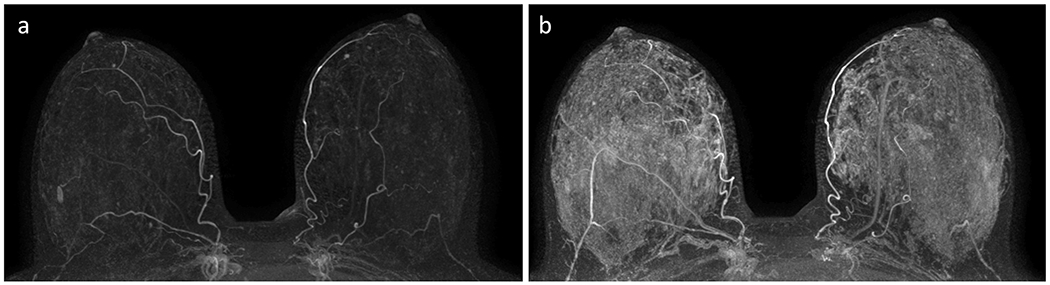
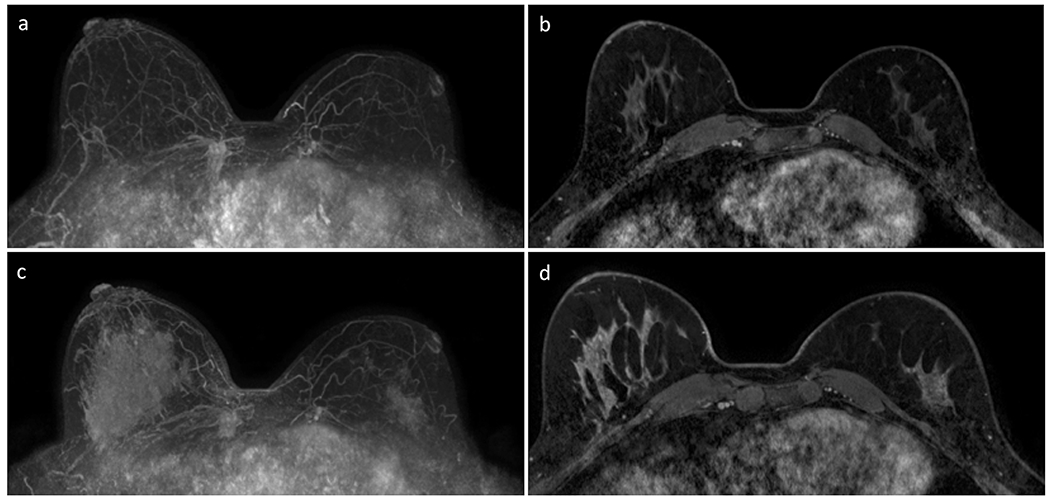
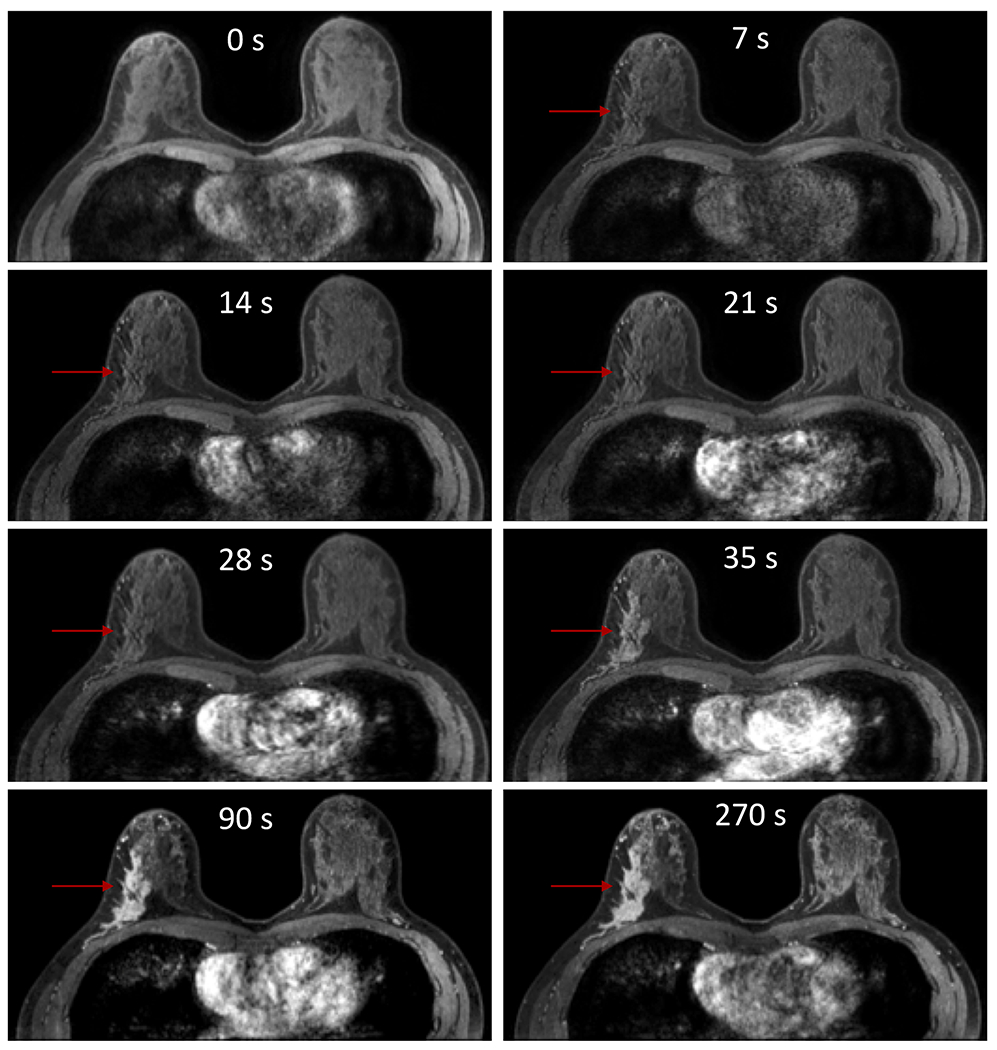
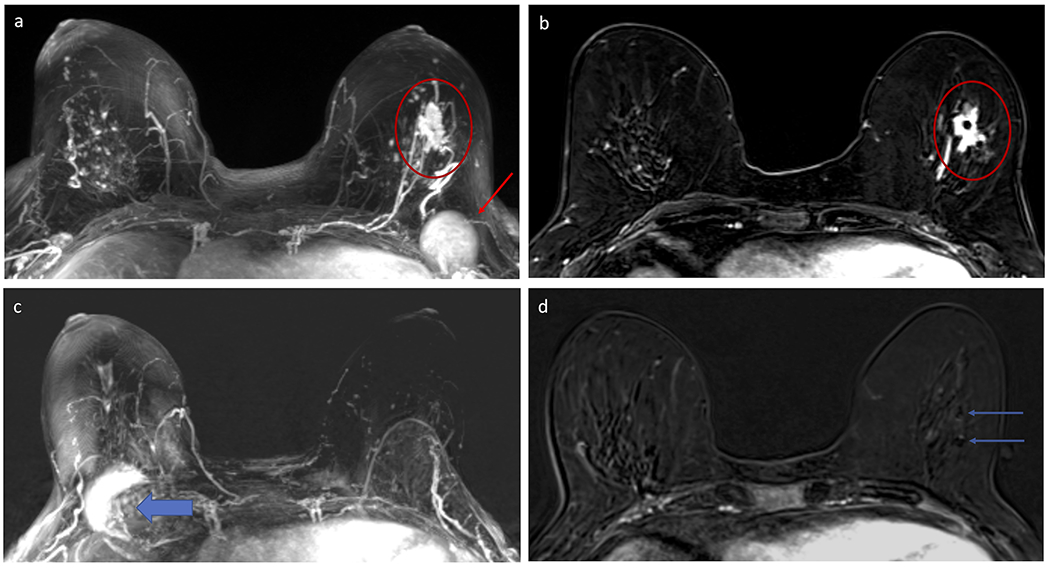
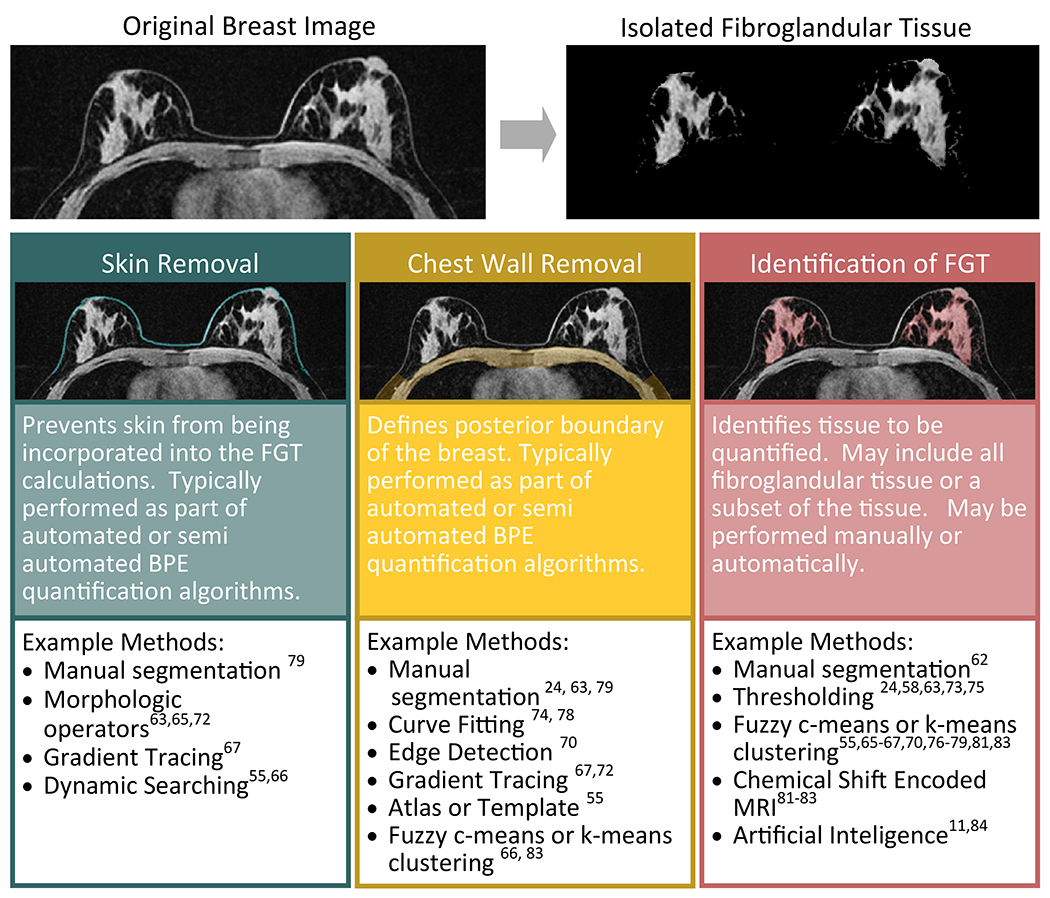
The degree of normal fibroglandular tissue that enhances on breast MRI, known as background parenchymal enhancement (BPE), was initially described as an incidental finding that could affect interpretation performance. While BPE is now established to be a physiologic phenomenon that is affected by both endogenous and exogenous hormone levels, evidence supporting the notion that BPE frequently masks breast cancers is limited. However, compelling data have emerged to suggest BPE is an independent marker of breast cancer risk and breast cancer treatment outcomes. Specifically, multiple studies have shown that elevated BPE levels, measured qualitatively or quantitatively, are associated with a greater risk of developing breast cancer. Evidence also suggests that BPE could be a predictor of neoadjuvant breast cancer treatment response and overall breast cancer treatment outcomes. These discoveries come at a time when breast cancer screening and treatment have moved toward an increased emphasis on targeted and individualized approaches, of which the identification of imaging features that can predict cancer diagnosis and treatment response is an increasingly recognized component. Historically, researchers have primarily studied quantitative tumor imaging features in pursuit of clinically useful biomarkers. However, the need to segment less well-defined areas of normal tissue for quantitative BPE measurements presents its own unique challenges. Furthermore, there is no consensus on the optimal timing on dynamic contrast-enhanced MRI for BPE quantitation. This article comprehensively reviews BPE with a particular focus on its potential to increase precision approaches to breast cancer risk assessment, diagnosis, and treatment. It also describes areas of needed future research, such as the applicability of BPE to women at average risk, the biological underpinnings of BPE, and the standardization of BPE characterization. Level of Evidence: 3 Technical Efficacy Stage: 5 J. Magn. Reson. Imaging 2020;51:43-61.
Keywords: background parenchymal enhancement; biomarkers; breast MRI; breast cancer risk; fibroglandular tissue; precision medicine.
© 2019 International Society for Magnetic Resonance in Medicine.
Figures
References
-
- Hortobagyi GN, Connolly JL, D’Orsi CJ, et al. AJCC cancer staging manual: Breast In: Amin MB, editor. AJCC cancer staging manual. Eight edition / editor-in-chief, Amin Mahul B. ; editors, Edge Stephen B. and 16 others ; Gress Donna M. - Technical editor ; Meyer Laura R. - Managing editor. ed. Chicago IL: American Joint Committee on Cancer, Springer; 2017. p. xvii, 1024 pages.
-
- Boyd NF, Byng JW, Jong RA, et al. Quantitative classification of mammographic densities and breast cancer risk: results from the Canadian National Breast Screening Study. J Natl Cancer Inst 1995;87(9):670–675. - PubMed
-
- Boyd NF, Guo H, Martin LJ, et al. Mammographic density and the risk and detection of breast cancer. N Engl J Med 2007;356(3):227–236. - PubMed
-
- Mandelson MT, Oestreicher N, Porter PL, et al. Breast density as a predictor of mammographic detection: comparison of interval- and screen-detected cancers. J Natl Cancer Inst 2000;92(13):1081–1087. - PubMed
-
- Barlow WE, White E, Ballard-Barbash R, et al. Prospective breast cancer risk prediction model for women undergoing screening mammography. J Natl Cancer Inst 2006;98(17):1204–1214. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
