

Copeptin and its role in the diagnosis of diabetes insipidus and the syndrome of inappropriate antidiuresis
- PMID: 31004513
- PMCID: PMC6850413
- DOI: 10.1111/cen.13991
Copeptin and its role in the diagnosis of diabetes insipidus and the syndrome of inappropriate antidiuresis
Abstract
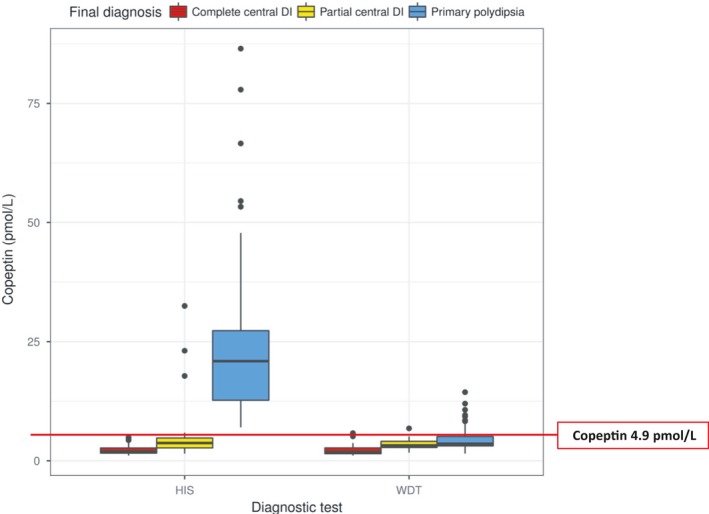
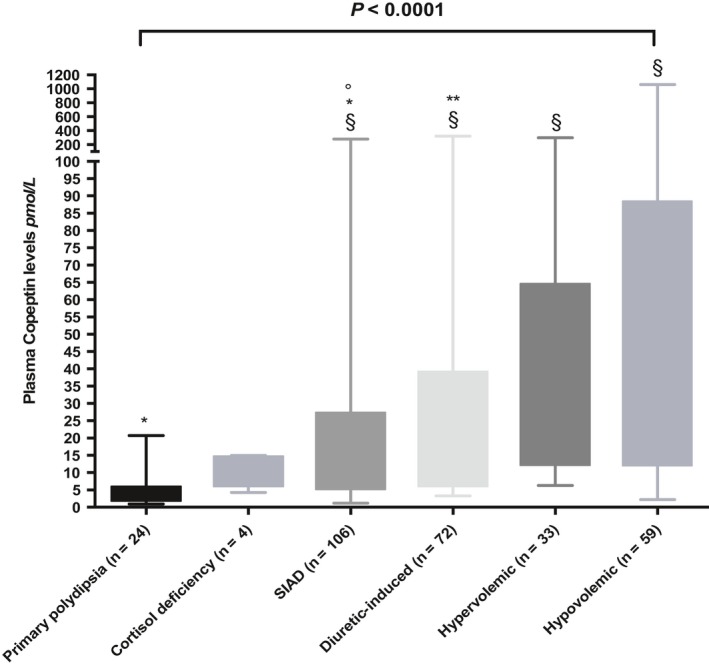
Copeptin is secreted in an equimolar amount to arginine vasopressin (AVP) but can easily be measured in plasma or serum with a sandwich immunoassay. The main stimuli for copeptin are similar to AVP, that is an increase in osmolality and a decrease in arterial blood volume and pressure. A high correlation between copeptin and AVP has been shown. Accordingly, copeptin mirrors the amount of AVP in the circulation. Copeptin has, therefore, been evaluated as diagnostic biomarker in vasopressin-dependent disorders of body fluid homeostasis. Disorders of body fluid homeostasis are common and can be divided into hyper- and hypoosmolar circumstances: the classical hyperosmolar disorder is diabetes insipidus, while the most common hypoosmolar disorder is the syndrome of inappropriate antidiuresis (SIAD). Copeptin measurement has led to a "revival" of the direct test in the differential diagnosis of diabetes insipidus. Baseline copeptin levels, without prior thirsting, unequivocally identify patients with nephrogenic diabetes insipidus. In contrast, for the difficult differentiation between central diabetes insipidus and primary polydipsia, a stimulated copeptin level of 4.9 pmol/L upon hypertonic saline infusion differentiates these two entities with a high diagnostic accuracy and is clearly superior to the classical water deprivation test. On the contrary, in the SIAD, copeptin measurement is of only little diagnostic value. Copeptin levels widely overlap in patients with hyponatraemia and emphasize the heterogeneity of the disease. Additionally, a variety of factors lead to unspecific copeptin elevations in the acute setting further complicating its interpretation. The broad use of copeptin as diagnostic marker in hyponatraemia and specifically to detect cancer-related disease in SIADH patients can, therefore, not be recommended.
Keywords: SIAD; copeptin; diabetes insipidus; diagnosis; hypernatremia; hyponatraemia; primary polydipsia.
© 2019 The Authors. Clinical Endocrinology Published by John Wiley & Sons Ltd.
Conflict of interest statement
All authors report no conflicts of interest.
Figures




References
-
- Verbalis JG. Disorders of body water homeostasis. Best Pract Res Clin Endocrinol Metab. 2003;17(4):471‐503. - PubMed
-
- Robertson GL. Diabetes insipidus. Endocrinol Metab Clin North Am. 1995;24(3):549‐572. - PubMed
-
- Kumar S, Berl T. Sodium. Lancet. 1998;352(9123):220‐228. - PubMed
-
- Upadhyay A, Jaber BL, Madias NE. Incidence and prevalence of hyponatremia. Am J Med. 2006;119(7 Suppl 1):S30‐S35. - PubMed
-
- Bartter FC, Schwartz WB. The syndrome of inappropriate secretion of antidiuretic hormone. Am J Med. 1967;42(5):790‐806. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
