

Psychotropic polypharmacy reconsidered: Between-class polypharmacy in the context of multimorbidity in the treatment of depressive disorders
- PMID: 31004825
- PMCID: PMC6520147
- DOI: 10.1016/j.jad.2019.04.018
Psychotropic polypharmacy reconsidered: Between-class polypharmacy in the context of multimorbidity in the treatment of depressive disorders
Abstract
Objectives: Both psychiatric polypharmacy and multimorbidity are common in depressed adults. We examine recent patterns of psychotropic polypharmacy with attention to concurrent multimorbidity in the treatment of depressive disorders in outpatient psychiatric care.
Methods: Data from the 2006-2015 National Ambulatory Medical Care Survey offer nationally representative samples of office-based psychiatric care in adults with depressive disorders (ICD-9-CM codes 296.20-296.26, 296.30-296.36, 300.4, 311, and 301.10-301.13) (n = 6,685 unweighted). These data allowed estimation of the prevalence of polypharmacy (within-class, between-class, and both) involving four major psychotropic classes: antidepressants, antipsychotics, mood-stabilizers, and sedative-hypnotics. We further evaluated the proportion of within-class and between-class psychotropic prescription combinations that were potentially justifiable, taking FDA-approved indications and multimorbidity into consideration.
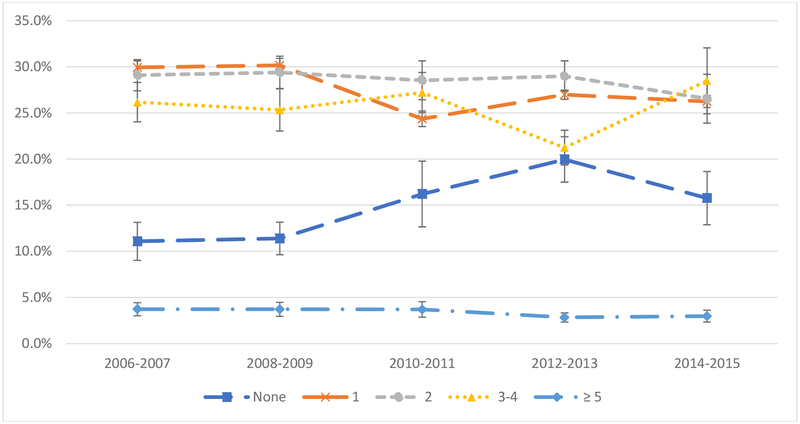
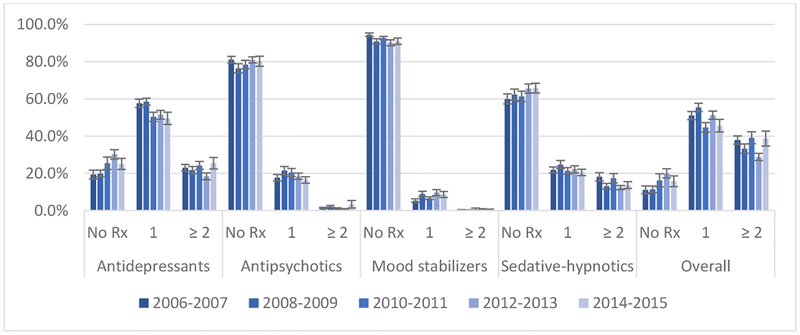
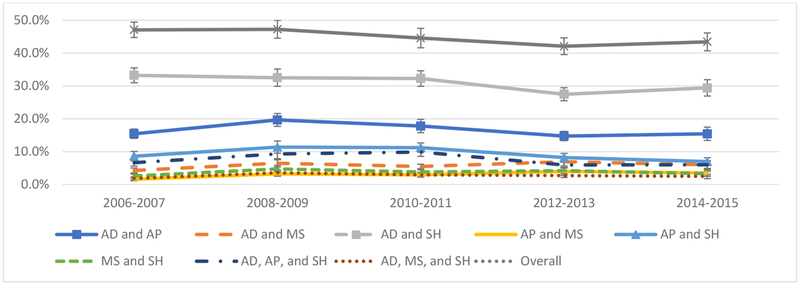
Results: Prescribing two or more psychotropic medications for depressed adults remained substantial and stable ranging from 59.0% in 2006-2007 to 58.0% in 2014-2015. The most common within-class polypharmacy types were: antidepressants (22.7%) and sedative-hypnotics (14.8%). The most common between-class polypharmacy types were: an antidepressant and a sedative-hypnotic (30.7%), an antidepressant and an antipsychotic (16.4%), and an antipsychotic and a sedative-hypnotic (9.0%). In visits in which between-class psychotropics were prescribed, 53.9% were potentially justified by FDA-approved augmentation and/or adjunctive treatment strategies or by psychiatric multimorbidities.
Conclusion: Psychotropic polypharmacy affects more than half of depressed adults. Between-class polypharmacy is the most common pattern and in over 50% of instances may be justified by augmentation strategies or considerations of psychiatric multimorbidity. Future research is needed to address effectiveness, safety, and cost-effectiveness of polypharmaceutical care for depression, especially those occurring with psychiatric co-morbididities.
Keywords: Depression; Pharmaco-epidemiology; Polypharmacy; Psychiatric co-morbidities; Psychotropics.
Copyright © 2019. Published by Elsevier B.V.
Figures
Similar articles
-
National trends in psychotropic medication polypharmacy in office-based psychiatry.Arch Gen Psychiatry. 2010 Jan;67(1):26-36. doi: 10.1001/archgenpsychiatry.2009.175. Arch Gen Psychiatry. 2010. PMID: 20048220
-
National trends in child and adolescent psychotropic polypharmacy in office-based practice, 1996-2007.J Am Acad Child Adolesc Psychiatry. 2010 Oct;49(10):1001-10. doi: 10.1016/j.jaac.2010.07.007. Epub 2010 Sep 1. J Am Acad Child Adolesc Psychiatry. 2010. PMID: 20855045 Free PMC article.
-
Effect of age on the profile of psychotropic users: results from the 2010 National Ambulatory Medical Care Survey.J Am Geriatr Soc. 2014 Feb;62(2):358-64. doi: 10.1111/jgs.12640. Epub 2014 Jan 13. J Am Geriatr Soc. 2014. PMID: 24417590
-
Psychotropic Drug Prescription in Children and Adolescents: Approved Medications in European Countries and the United States.J Child Adolesc Psychopharmacol. 2022 Mar;32(2):80-88. doi: 10.1089/cap.2021.0027. Epub 2022 Feb 9. J Child Adolesc Psychopharmacol. 2022. PMID: 35138922 Review.
-
A Clinical Review of the Use of Common Psychiatric Medications in Pregnancy: Guidelines for Obstetrical Providers.Obstet Gynecol Clin North Am. 2023 Mar;50(1):219-227. doi: 10.1016/j.ogc.2022.10.009. Obstet Gynecol Clin North Am. 2023. PMID: 36822705 Review.
Cited by
-
Association of Depression With 10-Year and Lifetime Cardiovascular Disease Risk Among US Adults, National Health and Nutrition Examination Survey, 2005-2018.Prev Chronic Dis. 2022 May 26;19:E28. doi: 10.5888/pcd19.210418. Prev Chronic Dis. 2022. PMID: 35617679 Free PMC article.
-
Pharmacotherapy, drug-drug interactions and potentially inappropriate medication in depressive disorders.PLoS One. 2021 Jul 22;16(7):e0255192. doi: 10.1371/journal.pone.0255192. eCollection 2021. PLoS One. 2021. PMID: 34293068 Free PMC article.
-
Psychotropic Polypharmacy in Adults 55 Years or Older: A Risk for Impaired Global Cognition, Executive Function, and Mobility.Front Pharmacol. 2020 Jan 30;10:1659. doi: 10.3389/fphar.2019.01659. eCollection 2019. Front Pharmacol. 2020. PMID: 32082159 Free PMC article.
-
Factors associated with drug-drug interactions involving citalopram in the UK Biobank.BJPsych Open. 2025 Aug 1;11(5):e166. doi: 10.1192/bjo.2025.10060. BJPsych Open. 2025. PMID: 40746135 Free PMC article.
-
Association between benzodiazepine anxiolytic polypharmacy and concomitant psychotropic medications in Japan: a retrospective cross-sectional study.Front Psychiatry. 2024 Jul 4;15:1405049. doi: 10.3389/fpsyt.2024.1405049. eCollection 2024. Front Psychiatry. 2024. PMID: 39026522 Free PMC article.
References
-
- World Health Organization. Depression: Fact sheet. 2017; http://www.who.int/mediacentre/factsheets/fs369/en/.
-
- Department of Veterans Affairs and Department of Defense. VA/DoD Clinical Practice Guideline for the Management of Major Depressive Disorder. 2016; https://www.healthquality.va.gov/guidelines/MH/mdd/MDDFullFinal5192016.pdf.
-
- Patkar AA, Pae CU. Atypical antipsychotic augmentation strategies in the context of guideline-based care for the treatment of major depressive disorder. CNS Drugs. 2013;27 Suppl 1:S29–37. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
