

Levetiracetam versus phenytoin for second-line treatment of paediatric convulsive status epilepticus (EcLiPSE): a multicentre, open-label, randomised trial
- PMID: 31005385
- PMCID: PMC6551349
- DOI: 10.1016/S0140-6736(19)30724-X
Levetiracetam versus phenytoin for second-line treatment of paediatric convulsive status epilepticus (EcLiPSE): a multicentre, open-label, randomised trial
Abstract
Background: Phenytoin is the recommended second-line intravenous anticonvulsant for treatment of paediatric convulsive status epilepticus in the UK; however, some evidence suggests that levetiracetam could be an effective and safer alternative. This trial compared the efficacy and safety of phenytoin and levetiracetam for second-line management of paediatric convulsive status epilepticus.
Methods: This open-label, randomised clinical trial was undertaken at 30 UK emergency departments at secondary and tertiary care centres. Participants aged 6 months to under 18 years, with convulsive status epilepticus requiring second-line treatment, were randomly assigned (1:1) using a computer-generated randomisation schedule to receive levetiracetam (40 mg/kg over 5 min) or phenytoin (20 mg/kg over at least 20 min), stratified by centre. The primary outcome was time from randomisation to cessation of convulsive status epilepticus, analysed in the modified intention-to-treat population (excluding those who did not require second-line treatment after randomisation and those who did not provide consent). This trial is registered with ISRCTN, number ISRCTN22567894.
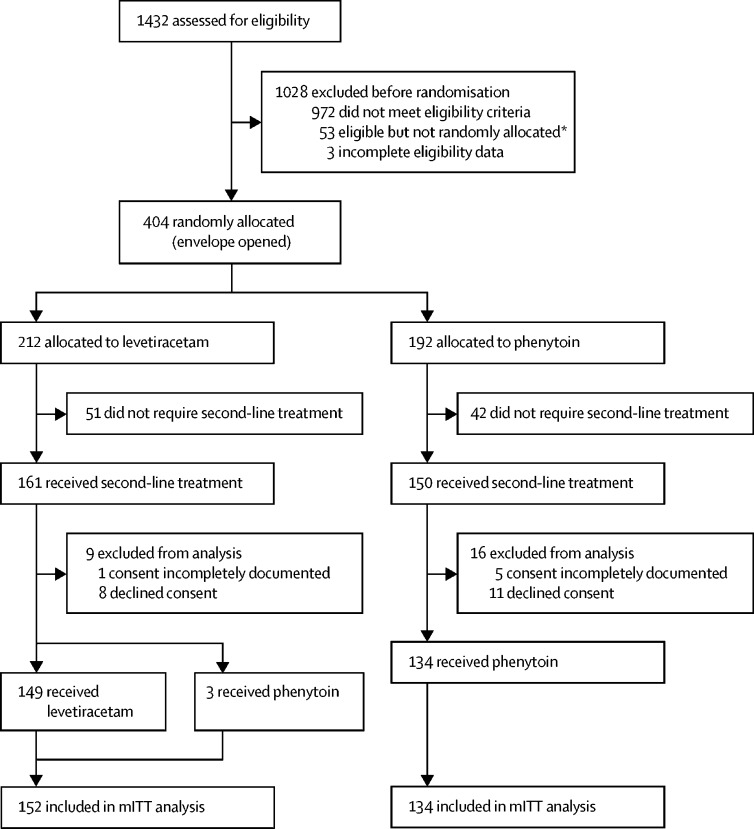
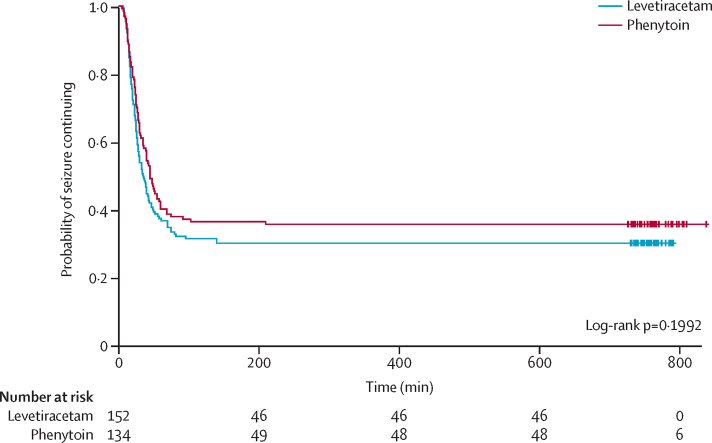
Findings: Between July 17, 2015, and April 7, 2018, 1432 patients were assessed for eligibility. After exclusion of ineligible patients, 404 patients were randomly assigned. After exclusion of those who did not require second-line treatment and those who did not consent, 286 randomised participants were treated and had available data: 152 allocated to levetiracetam, and 134 to phenytoin. Convulsive status epilepticus was terminated in 106 (70%) children in the levetiracetam group and in 86 (64%) in the phenytoin group. Median time from randomisation to cessation of convulsive status epilepticus was 35 min (IQR 20 to not assessable) in the levetiracetam group and 45 min (24 to not assessable) in the phenytoin group (hazard ratio 1·20, 95% CI 0·91-1·60; p=0·20). One participant who received levetiracetam followed by phenytoin died as a result of catastrophic cerebral oedema unrelated to either treatment. One participant who received phenytoin had serious adverse reactions related to study treatment (hypotension considered to be immediately life-threatening [a serious adverse reaction] and increased focal seizures and decreased consciousness considered to be medically significant [a suspected unexpected serious adverse reaction]).
Interpretation: Although levetiracetam was not significantly superior to phenytoin, the results, together with previously reported safety profiles and comparative ease of administration of levetiracetam, suggest it could be an appropriate alternative to phenytoin as the first-choice, second-line anticonvulsant in the treatment of paediatric convulsive status epilepticus.
Funding: National Institute for Health Research Health Technology Assessment programme.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Levetiracetam no better than phenytoin in children with convulsive status epilepticus.Lancet. 2019 May 25;393(10186):2101-2102. doi: 10.1016/S0140-6736(19)30896-7. Epub 2019 Apr 17. Lancet. 2019. PMID: 31005387 No abstract available.
-
Levetiracetam is a useful alternative to phenytoin for epileptic seizures in children.BMJ. 2019 Nov 11;367:l5464. doi: 10.1136/bmj.l5464. BMJ. 2019. PMID: 31712247
-
Phenytoin and levetiracetam are equally effective second-line treatments for status epilepticus.Arch Dis Child Educ Pract Ed. 2020 Oct;105(5):319-320. doi: 10.1136/archdischild-2019-318038. Epub 2019 Dec 11. Arch Dis Child Educ Pract Ed. 2020. PMID: 31826874 No abstract available.
References
-
- PICANet Annual Report 2010. PICANet. http://www.picanet.org.uk/Documentation
- PICANet Annual Report 2010. PICANet, http://www.picanet.org.uk/Documentation
-
- Metsäranta P, Koivikko M, Peltola J, Eriksson K. Outcome after prolonged convulsive seizures in 186 children: low morbidity, no mortality. Dev Med Child Neurol. 2004;46:4–8. - PubMed
- P Metsäranta, M Koivikko, J Peltola, K Eriksson. Outcome after prolonged convulsive seizures in 186 children: low morbidity, no mortality. Dev Med Child Neurol, 46, 2004, 4–8 - PubMed
-
- Chin RF, Neville BG, Peckham C, Bedford H, Wade A, Scott RC. Incidence, cause, and short-term outcome of convulsive status epilepticus in childhood: prospective population-based study. Lancet. 2006;368:222–229. - PubMed
- RF Chin, BG Neville, C Peckham, H Bedford, A Wade, RC Scott. Incidence, cause, and short-term outcome of convulsive status epilepticus in childhood: prospective population-based study. Lancet, 368, 2006, 222–229 - PubMed
-
- Hussain N, Appleton R, Thorburn K. Aetiology, course and outcome of children admitted to paediatric intensive care with convulsive status epilepticus: a retrospective 5-year review. Seizure. 2007;16:305–312. - PubMed
- N Hussain, R Appleton, K Thorburn. Aetiology, course and outcome of children admitted to paediatric intensive care with convulsive status epilepticus: a retrospective 5-year review. Seizure, 16, 2007, 305–312 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
