

Efficacy of Videostroboscopy and High-Speed Videoendoscopy to Obtain Functional Outcomes From Perioperative Ratings in Patients With Vocal Fold Mass Lesions
- PMID: 31005449
- PMCID: PMC6801021
- DOI: 10.1016/j.jvoice.2019.03.012
Efficacy of Videostroboscopy and High-Speed Videoendoscopy to Obtain Functional Outcomes From Perioperative Ratings in Patients With Vocal Fold Mass Lesions
Abstract
Objectives: A major limitation of comparing the efficacy of videostroboscopy (VS) and high-speed videoendoscopy (HSV) is the lack of an objective reference by which to compare the functional assessment ratings of the two techniques. For patients with vocal fold mass lesions, intraoperative measures of lesion size and depth may serve as this objective reference. This study compared the relationships between the pre- to postoperative change in VS and HSV visual-perceptual ratings to intraoperative measures of lesion size and depth.
Design: Prospective visual-perceptual study with intraoperative measures of lesion size and depth.
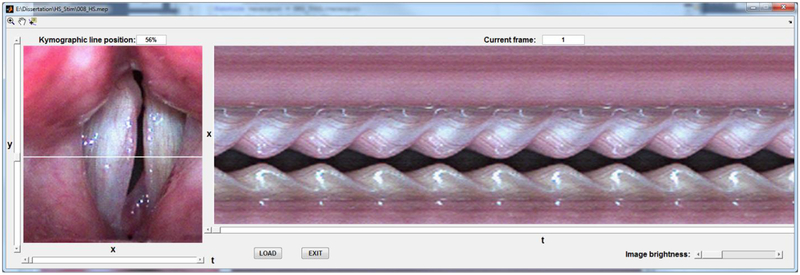
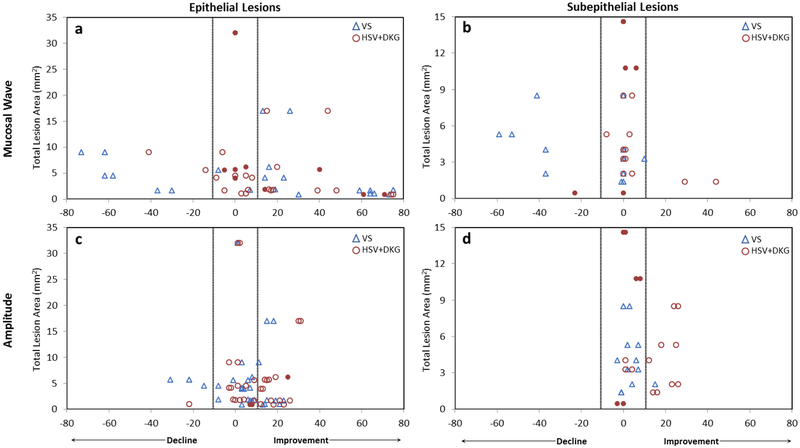
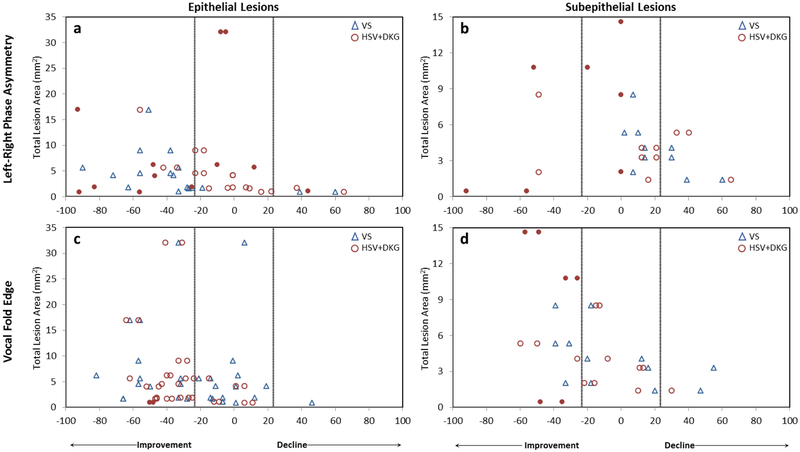
Methods: VS and HSV samples were obtained preoperatively and postoperatively from 28 patients with vocal fold lesions and from 17 vocally healthy controls. Two experienced clinicians rated amplitude, mucosal wave, vertical phase difference, left-right phase asymmetry, and vocal fold edge on a visual-analog scale using both imaging techniques. The change in perioperative ratings from VS and HSV was compared between groups and correlated to intraoperative measures of lesion size and depth.
Results: HSV was as reliable as VS for ratings of amplitude and edge, and substantially more reliable for ratings of mucosal wave and left-right phase asymmetry. Both VS and HSV had mild-moderate correlations between change in perioperative ratings and intraoperative measures of lesion area. Change in function could be obtained in more patients and for more parameters using HSV than VS. Group differences were noted for postoperative ratings of amplitude and edge; however, these differences were within one level of the visual-perceptual rating scale. The presence of asynchronicity in VS recordings renders vibratory features either uninterpretable or potentially distorted and thus should not be rated.
Conclusions: Amplitude and edge are robust vibratory measures for perioperative functional assessment, regardless of imaging modality. HSV is indicated for evaluation of subepithelial lesions or if asynchronicity is present in the VS image sequence.
Keywords: Assessment; High-speed videoendoscopy; Videostroboscopy; Vocal fold mass lesions; Voice disorders.
Copyright © 2019 The Voice Foundation. Published by Elsevier Inc. All rights reserved.
Figures


References
-
- Hillman RE, Montgomery WW, Zeitels SM. Appropriate use of objective measures of vocal function in the multidisciplinary management of voice disorders. Curr Opin Otolaryngol Head Neck Surg. 1997;5(3):172.
-
- Paul BC, Chen S, Sridharan S, Fang Y, Amin MR, Branski RC. Diagnostic accuracy of history, laryngoscopy, and stroboscopy. The Laryngoscope. 2013;123(1):215–219. - PubMed
-
- Hirano M, Bless DM. Videostroboscopic Examination of the Larynx. San Diego, Calif: Singular; 1993.
-
- Švec JG, Schutte HK. Videokymography: High-speed line scanning of vocal fold vibration. J Voice. 1996;10(2):201–205. - PubMed
-
- Švec J, Šram F, Schutte HK. Videokymography: A new high-speed method for the examination of vocal-fold vibrations. Otorinolaryngol Foniatr. 1999;48:155–162.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
