

Long-Term All-Cause and Cause-Specific Mortality in Asymptomatic Patients With CAC ≥1,000: Results From the CAC Consortium
- PMID: 31005541
- PMCID: PMC6745300
- DOI: 10.1016/j.jcmg.2019.02.005
Long-Term All-Cause and Cause-Specific Mortality in Asymptomatic Patients With CAC ≥1,000: Results From the CAC Consortium
Abstract
Objectives: This study thoroughly explored the demographic and imaging characteristics, as well as the all-cause and cause-specific mortality risks of patients with a coronary artery calcium (CAC) score ≥1,000 in the largest dataset of this population to date.
Background: CAC is commonly used to quantify cardiovascular risk. Current guidelines classify a CAC score of >300 or 400 as the highest risk group, yet little is known about the potentially unique imaging characteristics and mortality risk in individuals with a CAC score ≥1,000.
Methods: A total of 66,636 asymptomatic adults were included from the CAC consortium, a large retrospective multicenter clinical cohort. Mean patient follow-up was 12.3 ± 3.9 years for patients with cardiovascular disease (CVD), coronary heart disease (CHD), cancer, and all-cause mortality. Multivariate Cox proportional hazards regression models adjusted for age, sex, and conventional risk factors were used to assess the relative mortality hazard of individuals with CAC ≥1,000 compared with, first, a CAC reference of 0, and second, with patients with a CAC score of 400 to 999.
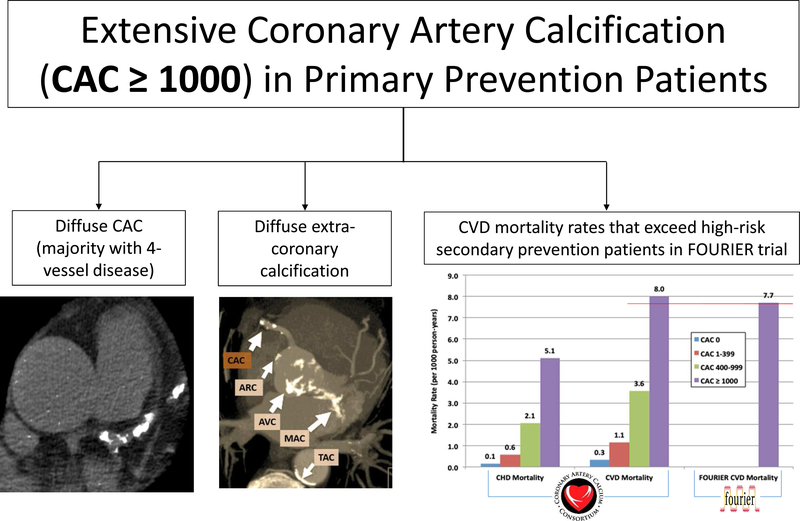
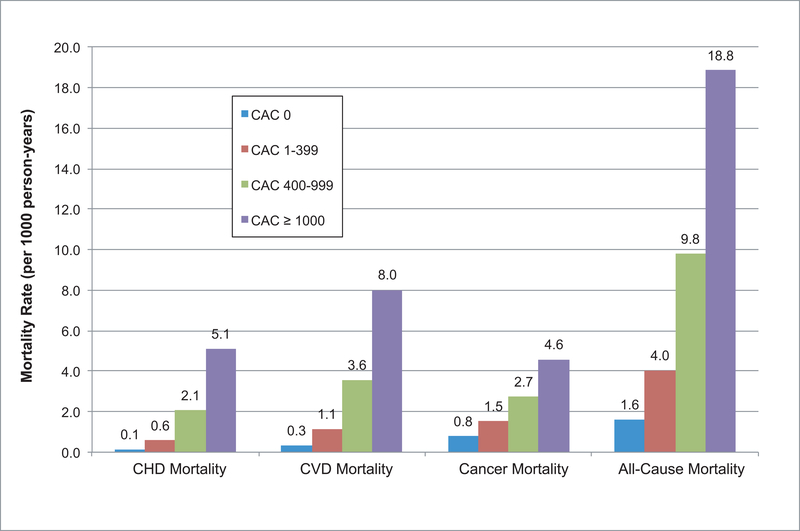
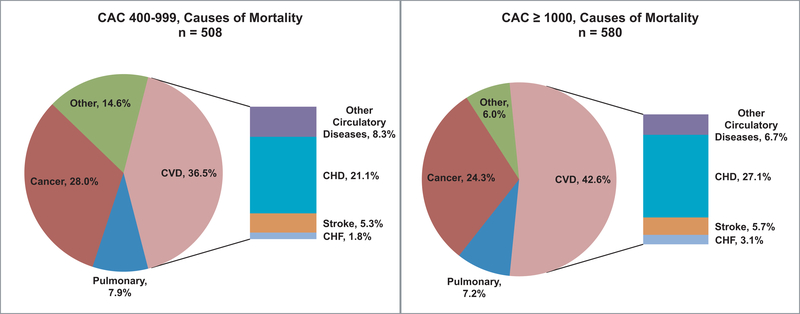
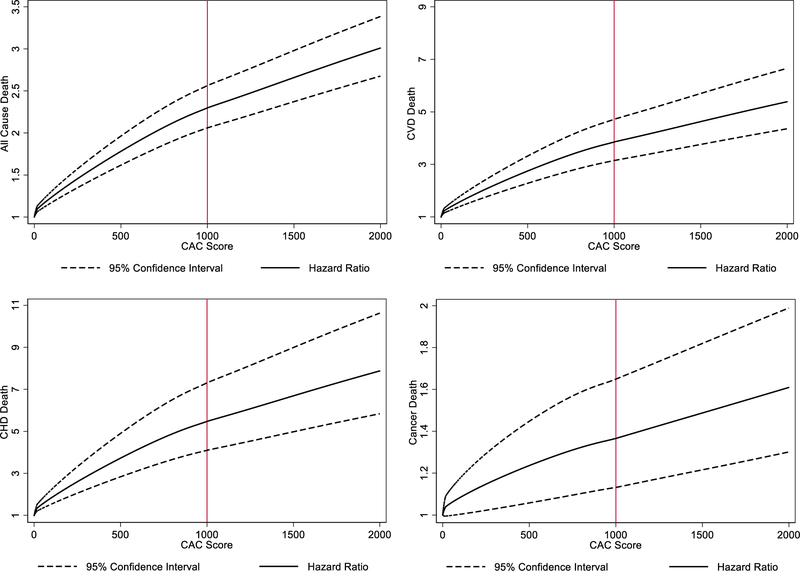
Results: There were 2,869 patients with CAC ≥1,000 (86.3% male, mean 66.3 ± 9.7 years of age). Most patients with CAC ≥1,000 had 4-vessel CAC (mean: 3.5 ± 0.6 vessels) and had greater total CAC area, higher mean CAC density, and more extracoronary calcium (79% with thoracic artery calcium, 46% with aortic valve calcium, and 21% with mitral valve calcium) than those with CAC scores of 400 to 999. After full adjustment, those with CAC ≥1,000 had a 5.04- (95% confidence interval [CI]: 3.92 to 6.48), 6.79- (95% CI: 4.74 to 9.73), 1.55- (95% CI:1.23 to 1.95), and 2.89-fold (95% CI: 2.53 to 3.31) risk of CVD, CHD, cancer, and all-cause mortality, respectively, compared to those with CAC score of 0. The CAC ≥1,000 group had a 1.71- (95% CI: 1.41 to 2.08), 1.84- (95% CI: 1.43 to 2.36), 1.36- (95% CI:1.07 to 1.73), and 1.51-fold (95% CI: 1.33 to 1.70) increased risk of CVD, CHD, cancer, and all-cause mortality compared to those with CAC scores 400 to 999. Graphic analysis of CAC ≥1,000 patients revealed continued logarithmic increase in risk, with no clear evidence of a risk plateau.
Conclusions: Patients with extensive CAC (CAC ≥1,000) represent a unique very high-risk phenotype with mortality outcomes commensurate with high-risk secondary prevention patients. Future guidelines should consider CAC ≥1,000 patients to be a distinct risk group who may benefit from the most aggressive preventive therapy.
Keywords: cardiovascular imaging; coronary artery calcium; high risk; primary prevention; risk scoring.
Copyright © 2020 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Coronary Artery Calcium: From the Power of 0 to >1,000.JACC Cardiovasc Imaging. 2020 Jan;13(1 Pt 1):94-96. doi: 10.1016/j.jcmg.2019.03.013. Epub 2019 Apr 17. JACC Cardiovasc Imaging. 2020. PMID: 31005522 No abstract available.
-
Extensive Coronary Artery Calcifications: No Longer Primary Prevention!JACC Cardiovasc Imaging. 2020 Jan;13(1 Pt 1):183-185. doi: 10.1016/j.jcmg.2019.12.007. JACC Cardiovasc Imaging. 2020. PMID: 31918909 No abstract available.
References
-
- Patel J et al. All-cause mortality in asymptomatic persons with extensive Agatston scores above 1000. Journal of Cardiovascular Computed Tomography 8, 26–32 (2014). - PubMed
-
- Hecht HS Coronary Artery Calcium Scanning: Past, Present, and Future. JACC: Cardiovascular Imaging 8, 579–596 (2015). - PubMed
