

Risk factors associated with revision for prosthetic joint infection following knee replacement: an observational cohort study from England and Wales
- PMID: 31005559
- PMCID: PMC6531378
- DOI: 10.1016/S1473-3099(18)30755-2
Risk factors associated with revision for prosthetic joint infection following knee replacement: an observational cohort study from England and Wales
Abstract
Background: Prosthetic joint infection is a devastating complication of knee replacement. The risk of developing a prosthetic joint infection is affected by patient, surgical, and health-care system factors. Existing evidence is limited by heterogeneity in populations studied, short follow-up, inadequate power, and does not differentiate early prosthetic joint infection, most likely related to the intervention, from late infection, more likely to occur due to haematogenous bacterial spread. We aimed to assess the overall and time-specific associations of these factors with the risk of revision due to prosthetic joint infection following primary knee replacement.
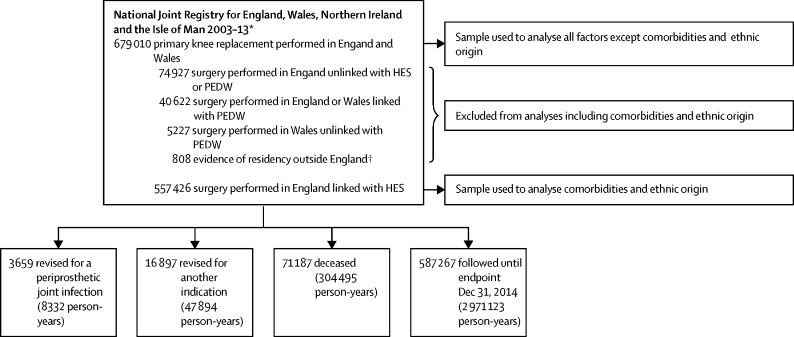
Methods: In this cohort study, we analysed primary knee replacements done between 2003 and 2013 in England and Wales and the procedures subsequently revised for prosthetic joint infection between 2003 and 2014. Data were obtained from the National Joint Registry linked to the Hospital Episode Statistics data in England and the Patient Episode Database for Wales. Each primary replacement was followed for a minimum of 12 months until the end of the observation period (Dec 31, 2014) or until the date of revision for prosthetic joint infection, revision for another indication, or death (whichever occurred first). We analysed the data using Poisson and piecewise exponential multilevel models to assess the associations between patient, surgical, and health-care system factors and risk of revision for prosthetic joint infection.
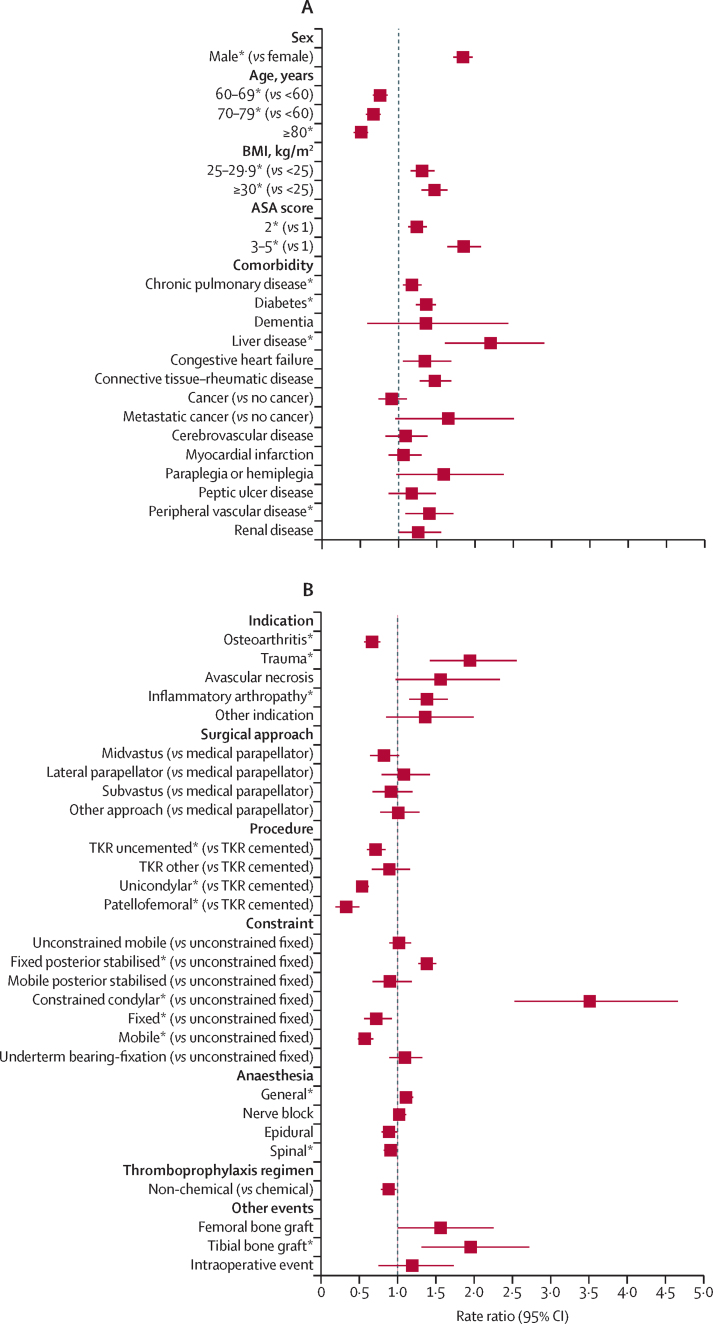
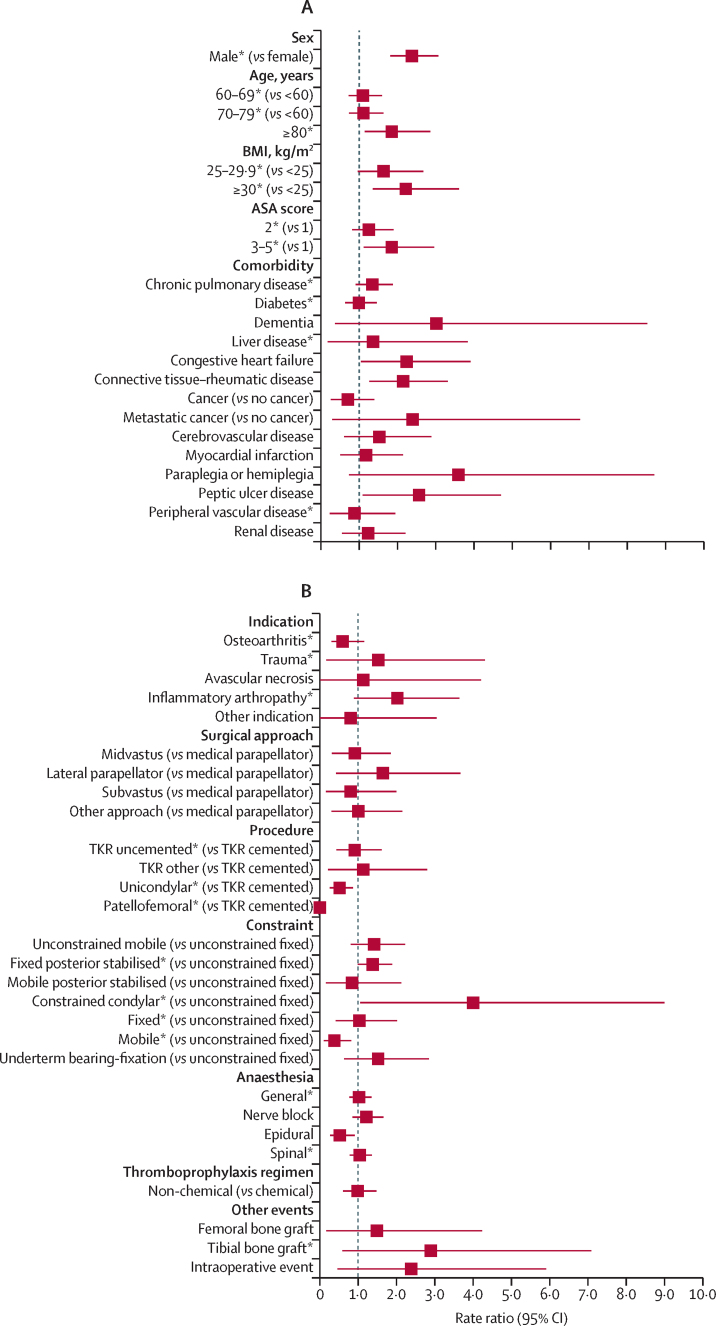
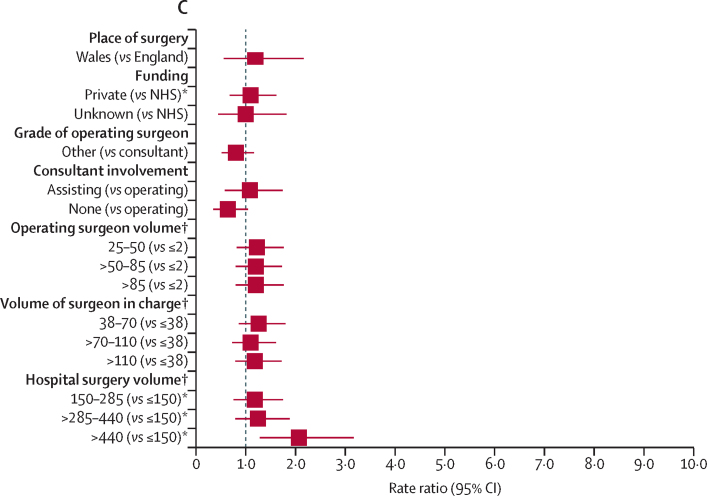
Findings: Of 679 010 primary knee replacements done between 2003 and 2013 in England and Wales, 3659 were subsequently revised for an indication of prosthetic joint infection between 2003 and 2014, after a median follow-up of 4·6 years (IQR 2·6-6·9). Male sex (rate ratio [RR] for male vs female patients 1·8 [95% CI 1·7-2·0]), younger age (RR for age ≥80 years vs <60 years 0·5 [0·4-0·6]), higher American Society of Anaesthesiologists [ASA] grade (RR for ASA grade 3-5 vs 1, 1·8 [1·6-2·1]), elevated body-mass index (BMI; RR for BMI ≥30 kg/m2vs <25 kg/m2 1·5 [1·3-1·6]), chronic pulmonary disease (RR 1·2 [1·1-1·3]), diabetes (RR 1·4 [1·2-1·5]), liver disease (RR 2·2 [1·6-2·9]), connective tissue and rheumatic diseases (RR 1·5 [1·3-1·7]), peripheral vascular disease (RR 1·4 [1·1-1·7]), surgery for trauma (RR 1·9 [1·4-2·6]), previous septic arthritis (RR 4·9 [2·7-7·6]) or inflammatory arthropathy (RR 1·4 [1·2-1·7]), operation under general anaesthesia (RR 1·1 [1·0-1·2]), requirement for tibial bone graft (RR 2·0 [1·3-2·7]), use of posterior stabilised fixed bearing prostheses (RR for posterior stabilised fixed bearing prostheses vs unconstrained fixed bearing prostheses 1·4 [1·3-1·5]) or constrained condylar prostheses (3·5 [2·5-4·7]) were associated with a higher risk of revision for prosthetic joint infection. However, uncemented total, patellofemoral, or unicondylar knee replacement (RR for uncemented vs cemented total knee replacement 0·7 [95% CI 0·6-0·8], RR for patellofemoral vs cemented total knee replacement 0·3 [0·2-0·5], and RR for unicondylar vs cemented total knee replacement 0·5 [0·5-0·6]) were associated with lower risk of revision for prosthetic joint infection. Most of these factors had time-specific effects, depending on the time period post-surgery.
Interpretation: We have identified several risk factors for revision for prosthetic joint infection following knee replacement. Some of these factors are modifiable, and the use of targeted interventions or strategies could lead to a reduced risk of revision for prosthetic joint infection. Non-modifiable factors and the time-specific nature of the effects we have observed will allow clinicians to appropriately counsel patients preoperatively and tailor follow-up regimens.
Funding: National Institute for Health Research.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Still fighting prosthetic joint infection after knee replacement.Lancet Infect Dis. 2019 Jun;19(6):560. doi: 10.1016/S1473-3099(19)30067-2. Epub 2019 Apr 17. Lancet Infect Dis. 2019. PMID: 31005558 No abstract available.
-
Risk factors associated with revision for prosthetic joint infection after knee replacement.Lancet Infect Dis. 2019 Aug;19(8):807. doi: 10.1016/S1473-3099(19)30357-3. Lancet Infect Dis. 2019. PMID: 31345449 No abstract available.
-
Risk factors associated with revision for prosthetic joint infection after knee replacement - Authors' reply.Lancet Infect Dis. 2019 Aug;19(8):807-808. doi: 10.1016/S1473-3099(19)30348-2. Lancet Infect Dis. 2019. PMID: 31345450 No abstract available.
References
-
- NJR Steering Commitee . National Joint Registry Centre; Hemel Hempstead: 2018. National Joint Registry for England, Wales, Northern Ireland and the Isle of Man: 15th annual report, 2017.
- NJR Steering Commite, ational Joint Registry for England, Wales, Northern Ireland and the Isle of Man: 15th annual report, 2017 201, 8 National Joint Registry Centr, emel Hempstead
-
- Blom AW, Brown J, Taylor AH, Pattison G, Whitehouse S, Bannister GC. Infection after total knee arthroplasty. J Bone Joint Surg Br. 2004;86:688–691. - PubMed
- AW Blom, J Brown, AH Taylor, G Pattison, S Whitehouse, GC Bannister. Infection after total knee arthroplasty. J Bone Joint Surg Br, 86, 2004, 688–691 - PubMed
-
- Nickinson RS, Board TN, Gambhir AK, Porter ML, Kay PR. The microbiology of the infected knee arthroplasty. Int Orthop. 2010;34:505–510. - PMC - PubMed
- RS Nickinson, TN Board, AK Gambhir, ML Porter, PR Kay. The microbiology of the infected knee arthroplasty. Int Orthop, 34, 2010, 505–510 - PMC - PubMed
-
- Boddapati V, Fu MC, Mayman DJ, Su EP, Sculco PK, McLawhorn AS. Revision total knee arthroplasty for periprosthetic joint infection is associated with increased postoperative morbidity and mortality relative to noninfectious revisions. J Arthroplasty. 2018;33:521–526. - PubMed
- V Boddapati, MC Fu, DJ Mayman, EP Su, PK Sculco, AS McLawhorn. Revision total knee arthroplasty for periprosthetic joint infection is associated with increased postoperative morbidity and mortality relative to noninfectious revisions. J Arthroplasty, 33, 2018, 521–526 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
