

Desmetramadol Has the Safety and Analgesic Profile of Tramadol Without Its Metabolic Liabilities: Consecutive Randomized, Double-Blind, Placebo- and Active Comparator-Controlled Trials
- PMID: 31005596
- PMCID: PMC6790288
- DOI: 10.1016/j.jpain.2019.04.005
Desmetramadol Has the Safety and Analgesic Profile of Tramadol Without Its Metabolic Liabilities: Consecutive Randomized, Double-Blind, Placebo- and Active Comparator-Controlled Trials
Abstract
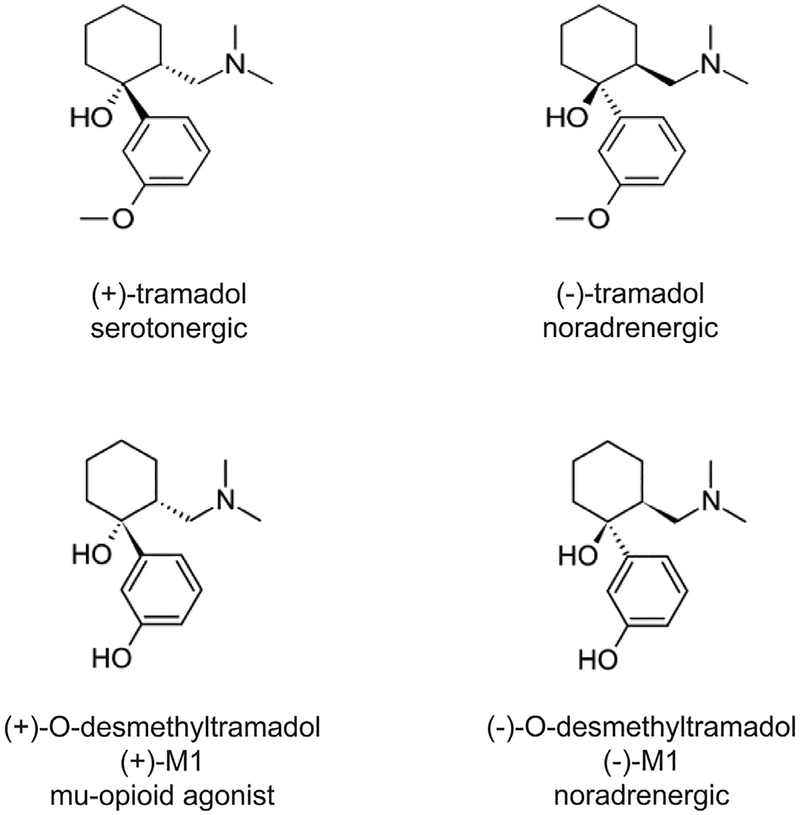
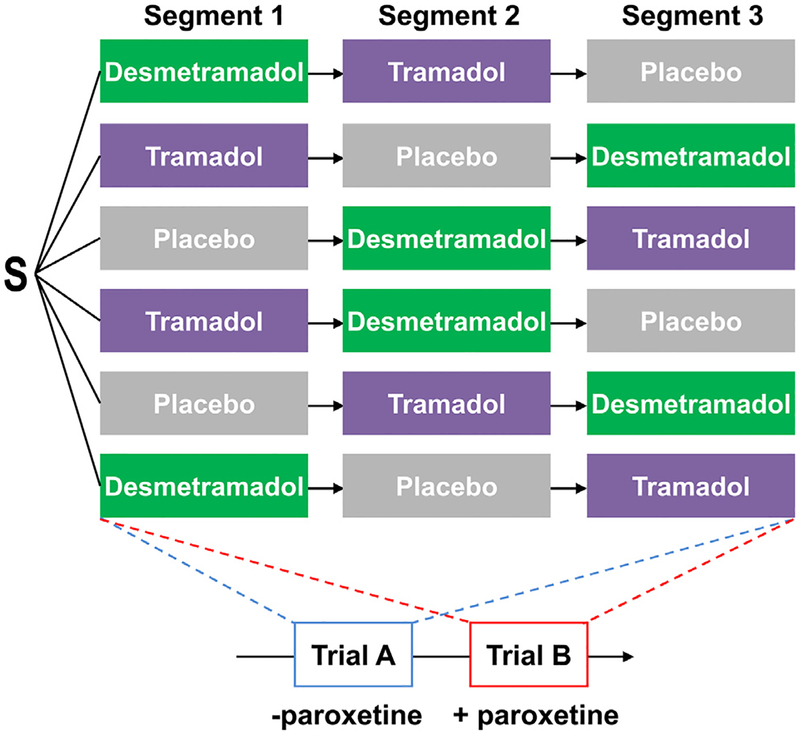
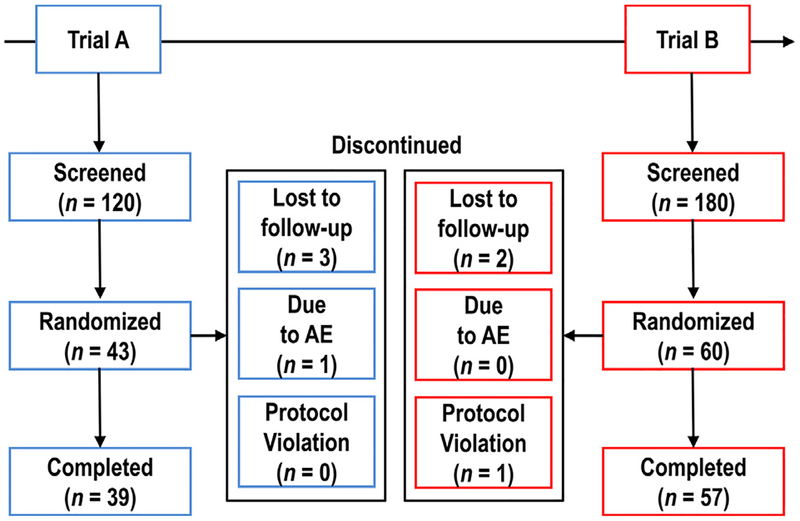
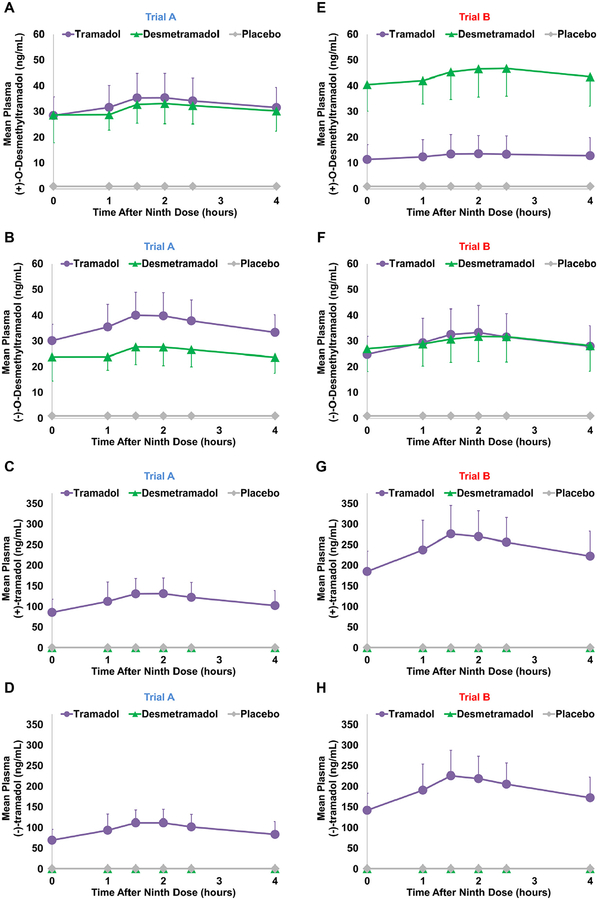
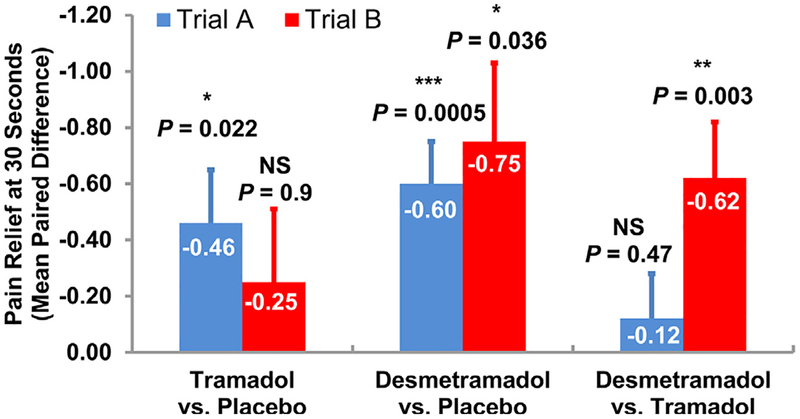
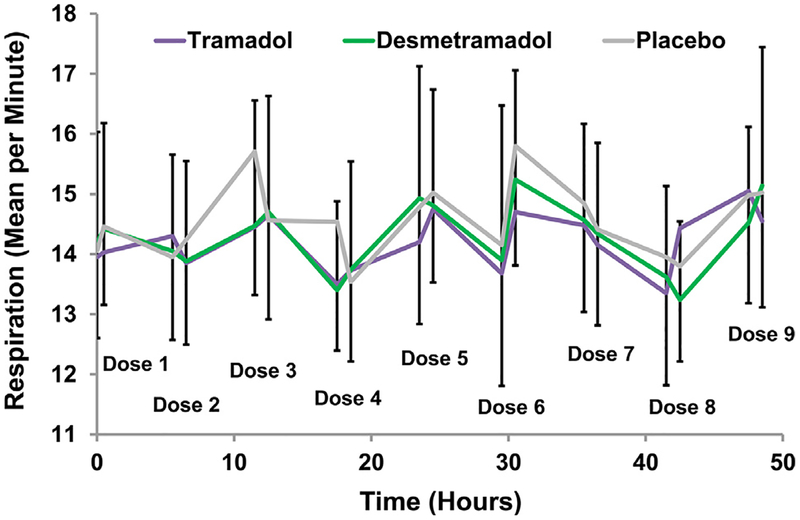
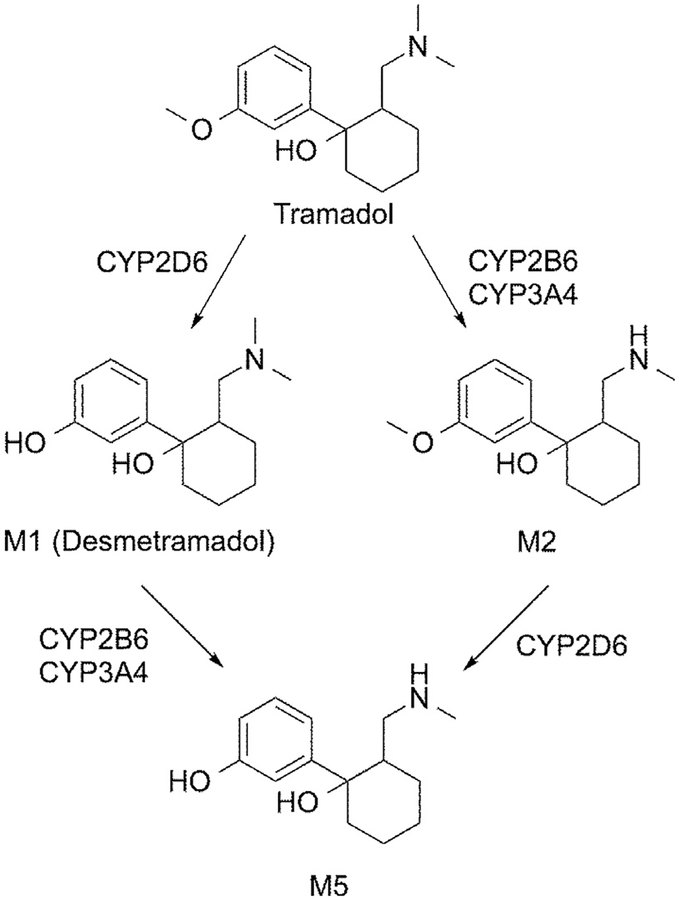
Desmetramadol is an investigational analgesic consisting of (+) and (-) enantiomers of the tramadol metabolite O-desmethyltramadol (M1). Tramadol is racemic and exerts analgesia by monoaminergic effects of (-)-tramadol and (-)-M1, and by the opioid (+)-M1. Tramadol labeling indicates cytochrome P450 (CYP) isozyme 2D6 ultrarapid metabolizer can produce dangerous (+)-M1 levels, and CYP2D6 poor metabolizers insufficient (+)-M1 for analgesia. We hypothesized that desmetramadol could provide the safety and analgesia of tramadol without its metabolic liabilities. We conducted consecutive double-blind, randomized, placebo-controlled, 3 segment cross-over trials A and B to investigate the steady-state pharmacokinetics and analgesia of 20 mg desmetramadol and 50 mg tramadol in 103 healthy participants without (n = 43) and with (n = 60) cotreatment with the CYP inhibitor paroxetine. In the absence of CYP inhibition (trial A), 20 mg desmetramadol and 50 mg tramadol dosed every 6 hours gave equivalent steady-state (+)-M1, similar adverse events, and analgesia significantly greater than placebo, but equal to each other. In trial B, CYP inhibition significantly depressed tramadol steady-state (+)-M1, reduced its adverse events, and led to insignificant analgesia comparable with placebo. In contrast, CYP inhibition in trial B had no deleterious effect on desmetramadol (+)-M1 or (-)-M1, which gave significant analgesia as in trial A and superior to tramadol (P = .003). Desmetramadol has the safety and efficacy of tramadol without its metabolic liabilities. CLINICALTRIALS.GOV REGISTRATIONS: NCT02205554, NCT03312777 PERSPECTIVE: To our knowledge, this is the first study of desmetramadol in humans and the first to show it provides the same safety and analgesia as tramadol, but without tramadol's metabolic liabilities and related drug-drug interactions. Desmetramadol could potentially offer expanded safety and usefulness to clinicians seeking an alternative to schedule II opioids.
Keywords: Desmetramadol; metabolism; poor metabolizer; tramadol; ultrarapid metabolizer.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Paroxetine, a cytochrome P450 2D6 inhibitor, diminishes the stereoselective O-demethylation and reduces the hypoalgesic effect of tramadol.Clin Pharmacol Ther. 2005 Apr;77(4):312-23. doi: 10.1016/j.clpt.2004.11.002. Clin Pharmacol Ther. 2005. PMID: 15903129 Clinical Trial.
-
Inhibition of CYP2D6-mediated tramadol O-demethylation in methadone but not buprenorphine maintenance patients.Br J Clin Pharmacol. 2012 Nov;74(5):835-41. doi: 10.1111/j.1365-2125.2012.04256.x. Br J Clin Pharmacol. 2012. PMID: 22369095 Free PMC article. Clinical Trial.
-
Tramadol as a new probe for cytochrome P450 2D6 phenotyping: a population study.Clin Pharmacol Ther. 2005 Jun;77(6):458-67. doi: 10.1016/j.clpt.2005.01.014. Clin Pharmacol Ther. 2005. PMID: 15961977
-
Trends in Tramadol: Pharmacology, Metabolism, and Misuse.Anesth Analg. 2017 Jan;124(1):44-51. doi: 10.1213/ANE.0000000000001683. Anesth Analg. 2017. PMID: 27861439 Review.
-
Clinical pharmacology of tramadol.Clin Pharmacokinet. 2004;43(13):879-923. doi: 10.2165/00003088-200443130-00004. Clin Pharmacokinet. 2004. PMID: 15509185 Review.
Cited by
-
Understanding Buprenorphine for Use in Chronic Pain: Expert Opinion.Pain Med. 2020 Apr 1;21(4):714-723. doi: 10.1093/pm/pnz356. Pain Med. 2020. PMID: 31917418 Free PMC article. Review.
-
Update on Treating Painful Diabetic Peripheral Neuropathy: A Review of Current US Guidelines with a Focus on the Most Recently Approved Management Options.J Pain Res. 2024 Mar 13;17:1005-1028. doi: 10.2147/JPR.S442595. eCollection 2024. J Pain Res. 2024. PMID: 38505500 Free PMC article. Review.
-
Centrally administered CYP2D inhibitors increase oral tramadol analgesia in rats.Brain Res Bull. 2020 Nov;164:400-406. doi: 10.1016/j.brainresbull.2020.09.001. Epub 2020 Sep 11. Brain Res Bull. 2020. PMID: 32926950 Free PMC article.
-
Desmetramadol Is Identified as a G-Protein Biased µ Opioid Receptor Agonist.Front Pharmacol. 2020 Jan 30;10:1680. doi: 10.3389/fphar.2019.01680. eCollection 2019. Front Pharmacol. 2020. PMID: 32116679 Free PMC article.
-
The Oxford Catalogue of Opioids: A systematic synthesis of opioid drug names and their pharmacology.Br J Clin Pharmacol. 2021 Oct;87(10):3790-3812. doi: 10.1111/bcp.14786. Epub 2021 Mar 20. Br J Clin Pharmacol. 2021. PMID: 33608948 Free PMC article.
References
-
- Bianchi AL, Denavit-Saubie M, Champagnat J: Central control of breathing in mammals: Neuronal circuitry, membrane properties, and neurotransmitters. Physiol Rev 75:1–45, 1995 - PubMed
-
- Bloch MB, Dyer RA, Heijke SA, James MF: Tramadol infusion for postthoracotomy pain relief: A placebo-controlled comparison with epidural morphine. Anesthes Analges 94:523–528, 2002 - PubMed
-
- Bolme P, Corrodi H, Fuxe K, Hokfelt T, Lidbrink P, Goldstein M: Possible involvement of central adrenaline neurons in vasomotor and respiratory control. Studies with clonidine and its interactions with piperoxane and yohimbine. Eur J Pharmacol 28:89–94, 1974 - PubMed
-
- Champagnat J, Denavit-Saubie M, Henry JL, Leviel V: Catecholaminergic depressant effects on bulbar respiratory mechanisms. Brain Res 160:57–68, 1979 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
