

Yield of Clinical Screening for Hypertrophic Cardiomyopathy in Child First-Degree Relatives
- PMID: 31006259
- PMCID: PMC6636798
- DOI: 10.1161/CIRCULATIONAHA.118.038846
Yield of Clinical Screening for Hypertrophic Cardiomyopathy in Child First-Degree Relatives
Abstract
Background: Hypertrophic cardiomyopathy (HCM) is a heritable myocardial disease with age-related penetrance. Current guidelines recommend clinical screening of relatives beginning at 10 years of age, but the clinical value of this approach has not been systematically evaluated.
Methods: Anonymized clinical data were collected from children referred for family screening between 1994 and 2017 after diagnosis of HCM in a first-degree relative.
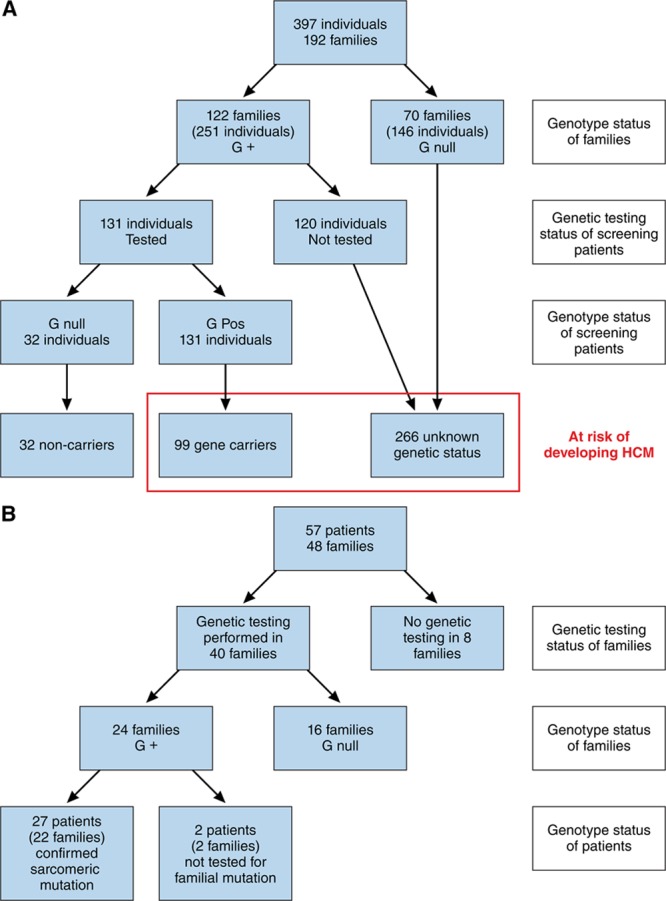
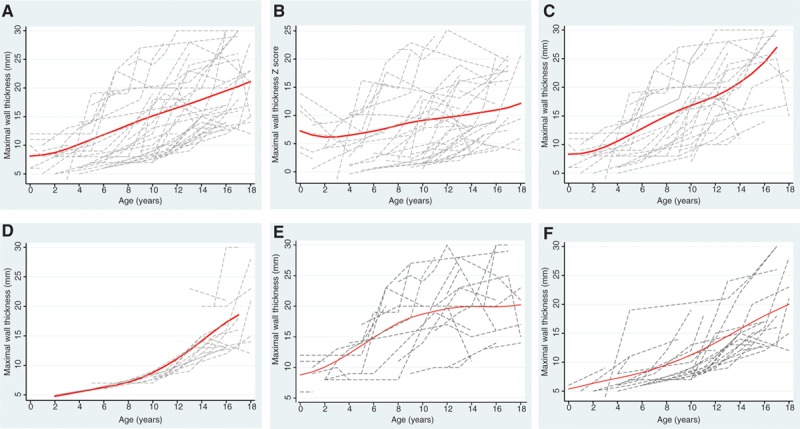
Results: Of 1198 consecutive children (≤18 years of age) from 594 families who underwent serial evaluation (median, 3.5 years; interquartile range, 1.2-7), 32 individuals met diagnostic criteria at baseline (median maximal left ventricular wall thickness, 13 mm; interquartile range, 8-21 mm), and 25 additional patients developed HCM during follow-up. Median age at diagnosis was 10 years (interquartile range, 4-13 years); 44 (72%) were ≤12 years of age. Median age of affected patients at the last follow-up was 14 years (interquartile range, 9.5-18.2 years). A family history of childhood HCM was more common in those patients diagnosed with HCM (n=32 [56%] versus n=257 [23%]; P<0.001). Eighteen patients (32%) were started on medication for symptoms; 2 (4%) underwent a septal myectomy; 14 (25%) received an implantable cardioverter-defibrillator; 1 underwent cardiac transplantation; 2 had a resuscitated cardiac arrest; and 1 died after a cerebrovascular accident.
Conclusions: Almost 5% of first-degree child relatives undergoing screening meet diagnostic criteria for HCM at first or subsequent evaluations, with the majority presenting as preadolescents; a diagnosis in a child first-degree relative is made in 8% of families screened. The phenotype of familial HCM in childhood is varied and includes severe disease, suggesting that clinical screening should begin at a younger age.
Keywords: cardiomyopathies; child; death, sudden; genetics; mass screening.
Figures
Comment in
-
To Screen or Not to Screen, That Is the Question.Circulation. 2019 Jul 16;140(3):193-195. doi: 10.1161/CIRCULATIONAHA.119.041021. Epub 2019 Jul 15. Circulation. 2019. PMID: 31306063 No abstract available.
References
-
- Arola A, Jokinen E, Ruuskanen O, Saraste M, Pesonen E, Kuusela AL, Tikanoja T, Paavilainen T, Simell O. Epidemiology of idiopathic cardiomyopathies in children and adolescents: a nationwide study in Finland. Am J Epidemiol. 1997;146:385–393. doi: 10.1093/oxfordjournals.aje.a009291. - PubMed
-
- Lipshultz SE, Sleeper LA, Towbin JA, Lowe AM, Orav EJ, Cox GF, Lurie PR, McCoy KL, McDonald MA, Messere JE, Colan SD. The incidence of pediatric cardiomyopathy in two regions of the United States. N Engl J Med. 2003;348:1647–1655. doi: 10.1056/NEJMoa021715. - PubMed
-
- Nugent AW, Daubeney PE, Chondros P, Carlin JB, Cheung M, Wilkinson LC, Davis AM, Kahler SG, Chow CW, Wilkinson JL, Weintraub RG National Australian Childhood Cardiomyopathy Study. The epidemiology of childhood cardiomyopathy in Australia. N Engl J Med. 2003;348:1639–1646. doi: 10.1056/NEJMoa021737. - PubMed
-
- Nugent AW, Daubeney PE, Chondros P, Carlin JB, Colan SD, Cheung M, Davis AM, Chow CW, Weintraub RG National Australian Childhood Cardiomyopathy Study. Clinical features and outcomes of childhood hypertrophic cardiomyopathy: results from a national population-based study. Circulation. 2005;112:1332–1338. doi: 10.1161/CIRCULATIONAHA.104.530303. - PubMed
-
- Colan SD, Lipshultz SE, Lowe AM, Sleeper LA, Messere J, Cox GF, Lurie PR, Orav EJ, Towbin JA. Epidemiology and cause-specific outcome of hypertrophic cardiomyopathy in children: findings from the Pediatric Cardiomyopathy Registry. Circulation. 2007;115:773–781. doi: 10.1161/CIRCULATIONAHA.106.621185. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
